Article Text

Statistics from Altmetric.com
Description
A woman aged 40 years affected by an aggressive and active form of rheumatoid arthritis (RA) underwent total knee arthroplasty (TKA) of the left knee for persistent synovitis after several therapeutic lines, the last one included methotrexate and a TNF-inhibitor.
Two months after the surgical procedure, the patient reported mild fever and persistent swelling of the left knee. On examination, there were signs of inflammation but no effusion to drain. Ultrasonography only showed oedema of the tissues surrounding the knee, and therefore, suspecting a prosthetic infection, antibiotic therapy was immediately started.
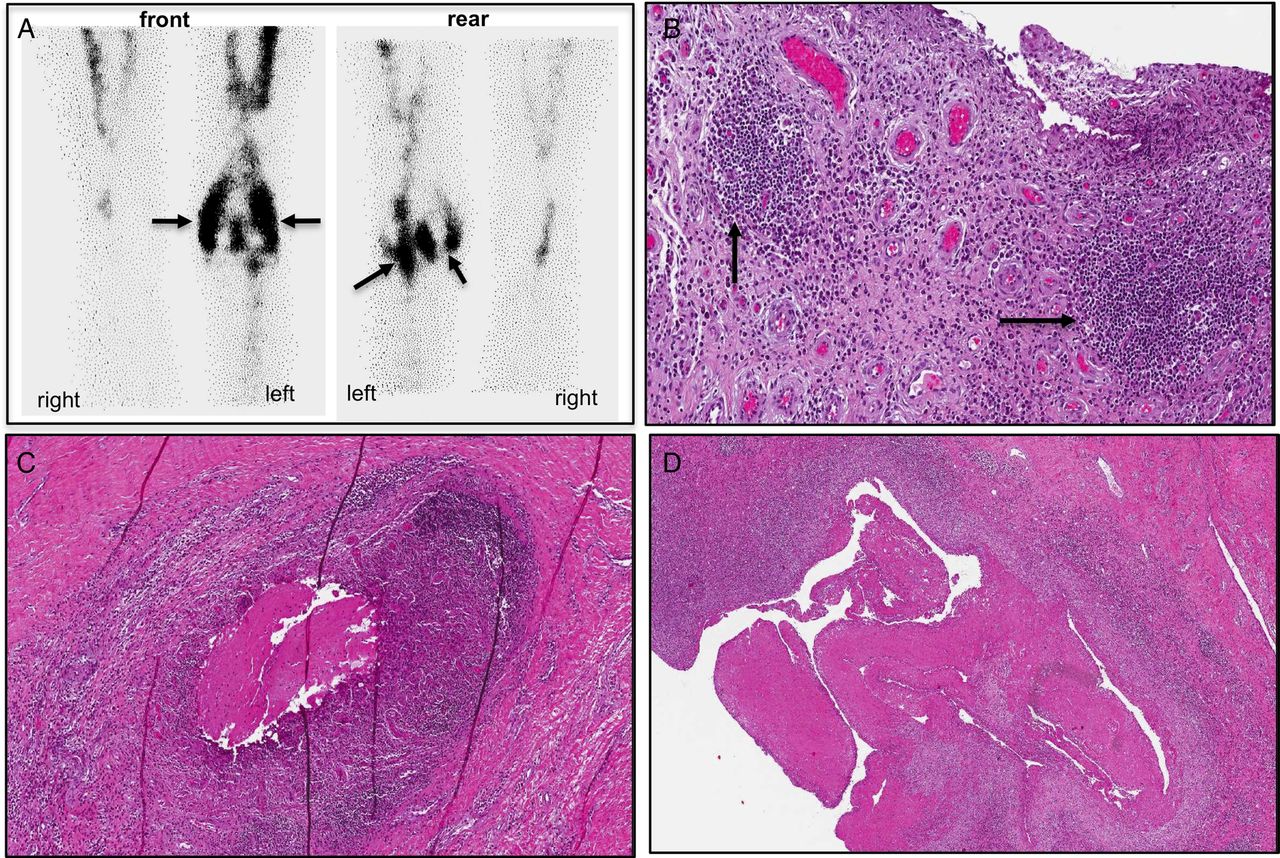
A subsequent scintigraphy with 99mTC-HmPAO (hexamethylpropylene-amine-oxime)-labelled leucocytes demonstrated the presence of early and persistent accumulation of labelled leucocytes in the femoral and tibial periprosthetic soft tissues, supporting the hypothesis of prosthetic infection (figure 1A).

{kind=link}
(A) Images of the scintigraphy with 99mTC-HmPAO (hexamethylpropylene-amine-oxime)-labelled leucocytes, showing early and persistent (after 4 hours) accumulation (black arrows) of labelled leucocytes in the femoral and tibial periprosthetic space and in periarticular soft tissues, particularly in the rear of the left knee. (B) The surgical specimen is represented by iuxta-articular fibro-fatty soft tissues infiltrated by plasma cells and lymphocytes, with the presence of lymphoid follicles (black arrows). Rheumatoid nodules are also evident; they are composed of a necrotic centre impregnated with fibrin, surrounded by a predominantly histiocytic inflammatory reaction, often arranged in a palisading fashion (C and D).
Empiric therapy with different lines of broad-spectrum antibiotics was continued for another month without benefit.
A revision surgery of the left knee was therefore performed and the histopathological examination of the surgical specimen demonstrated lymphocytic and plasmacellular infiltration in the periarticular soft tissues and the presence of rheumatoid nodules, without active synovitis (figure 1B–D).
A diagnosis of extra-articular RA recurrence sustained by rheumatoid nodules within the soft tissues surrounding the prosthetic joint was made.
Extra-articular RA recurrence after TKA was previously described and usually presents with rheumatoid nodules, lymphoplasmacytic infiltration and/or proliferation of synovial stromal cells.1 ,2
Though infection represents the primary suspicion in immunosuppressed patients, especially those taking a TNF-inhibitor,3 the possibility of an extra-articular RA recurrence mimicking infection after prosthetic surgery should be considered in the differential diagnosis.
Learning points
Immunosuppressive treatment in rheumatoid arthritis (RA) patients raised concern of septic complications in patients undergoing surgery.
Periprosthetic RA recurrence should be considered in the differential diagnosis of suspected septic arthritis after elective joint surgery.
Periprosthetic RA recurrence should be accounted like a real RA flare and treated consequently.
Footnotes
Contributors MML and DB have contributed significantly in conception and design, acquisition and interpretation of data, drafting the article and revising the manuscript for important intellectual content. MR contributed in acquisition and interpretation of data. AG contributed in analysis and interpretation of data and revision of the manuscript for important intellectual content. All authors gave final approval of the version to be published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.