Article Text

Summary
The most common histological classification of bile duct cancer is adenocarcinoma and squamous cell carcinoma (SCC) is relatively rare. We report a case of a 78-year-old man with SCC of the extrahepatic bile duct associated with metachronous para-aortic lymph node metastasis. He had undergone subtotal stomach-preserving pancreatoduodenectomy. The pathological findings demonstrated moderately differentiated SCC of the distal extrahepatic bile duct (T1N1M0, stage IIB). 6 months after surgery, recurrence of the para-aortic lymph node was shown in abdominal CT. 5 courses of tegafur/gimeracil/oteracil (S-1) plus cisplatin therapy was performed and the para-aortic lymph node disappeared, confirmed as complete response by imaging findings. The patient is alive without recurrence, 10 months after recurrence and chemotherapy.
Statistics from Altmetric.com
Background
Squamous cell carcinoma (SCC) of the bile duct is a rare tumour, first reported by Cabot1 in 1930. Since then, only 13 cases of SCC originating in the extrahepatic bile duct have been reported. We here report a case of SCC of the extrahepatic bile duct associated with metachronous para-aortic lymph node metastasis in a 78-year-old Japanese man who was managed with a pancreatoduodenectomy (PD) and chemotherapy.
Case presentation
A 78-year-old man presented with a 2-week history of brown urine. On his regular clinic visits, jaundice was pointed out and was admitted to our hospital for a detailed examination. Physical examination revealed scleral icterus without abdominal pain or fever. The patient's medical history included arteriosclerosis obliterans, hypertension and epilepsy. He had neither occupational history to the printing industry nor any appreciable family history.
Investigations
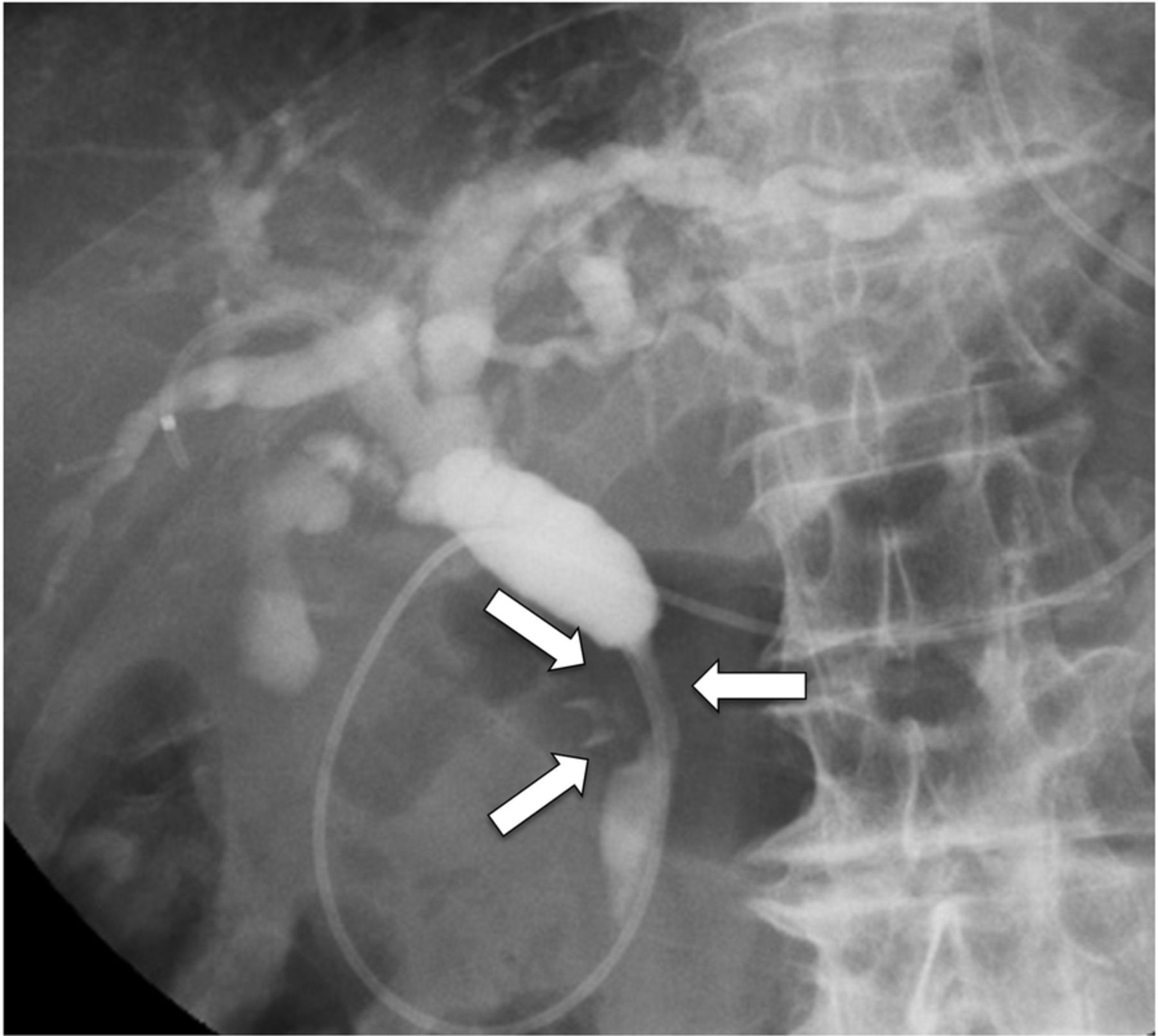
Laboratory data showed mild anaemia, obstructive jaundice and elevated hepatobiliary enzyme activities. Serum levels of CEA, CA19-9 and DUPAN-2 were normal (4.3 ng/mL, 8.0 U/mL and 133 U/mL, respectively). Abdominal CT revealed luminal narrowing of the distal bile duct with wall thickening and enhancement (figure 1A). There was no lymph node metastasis in the para-aortic region (figure 5A). The distal bile duct was shown as a low signal intensity area in T2-weighted MRI and high signal intensity area in diffusion-weighed image (figure 1B). On endoscopic retrograde cholangiopancreatography, there was a luminal narrowing (2 cm in length) in the distal bile duct with proximal dilation (figure 2). Bile cytology revealed atypical squamous cells of keratinising type with high nucleus–cytoplasm ratio, diagnosed as SCC. Additional blood examination showed increased serum levels of SCC 10.7 ng/mL (normal range <1.5 ng/mL) and CYFRA 3.7 ng/mL (normal range <2.0 ng/mL).

(A) Abdominal CT revealed luminal narrowing of the distal bile duct with wall thickening and enhancement (black arrow). (B) MRI findings showed a low signal intensity area in T2-weighted image (white arrow) and high signal intensity area in DWI. (C) Magnetic resonance cholangiopancreatography findings showed a luminal narrowing in the distal bile duct (arrow heads) with proximal dilation. DWI, diffusion-weighed image.

ERCP findings showed a luminal narrowing (2 cm in length) in the distal bile duct (arrows) with proximal dilation. ERCP, endoscopic retrograde cholangiopancreatography.
Treatment
The patient underwent subtotal stomach-preserving pancreatoduodenectomy (SSPPD) with lymph node dissection. At laparotomy, a hard mass was found in the distal bile duct without invasion to the surrounding tissues or vessels.
Outcome and follow-up
The resected specimen measured 30×20 mm and exhibited the nodular-infiltrating type (figure 3A). Histopathologically, sheets of atypical cells infiltrating into the fibromuscular (FM) layer were shown with no components of adenocarcinoma (figure 4A). Cancer pearls and keratinised cells with intercellular bridges were found suggesting moderately differentiated SCC (figure 4B). One out of 34 regional lymph nodes (anterosuperior lymph node along the common hepatic artery) when dissected showed SCC metastasis. Based on these findings, a definitive diagnosis of SCC of the distal extrahepatic bile duct was made.

(A) Microscopic findings of the resected specimen measured 30×20 mm and exhibited the nodular-infiltrating type (arrow heads). (B and C) Serial sections at 4–6 mm intervals were prepared from the entire area of the extrahepatic bile duct.

Microscopic findings ((A) H&E: ×40; (B): ×200). (A) Sheets of atypical cells infiltrating to the fibromuscular layer were shown without components of adenocarcinoma. (B) Cancer pearls and keratinised cells with intercellular bridges were found.
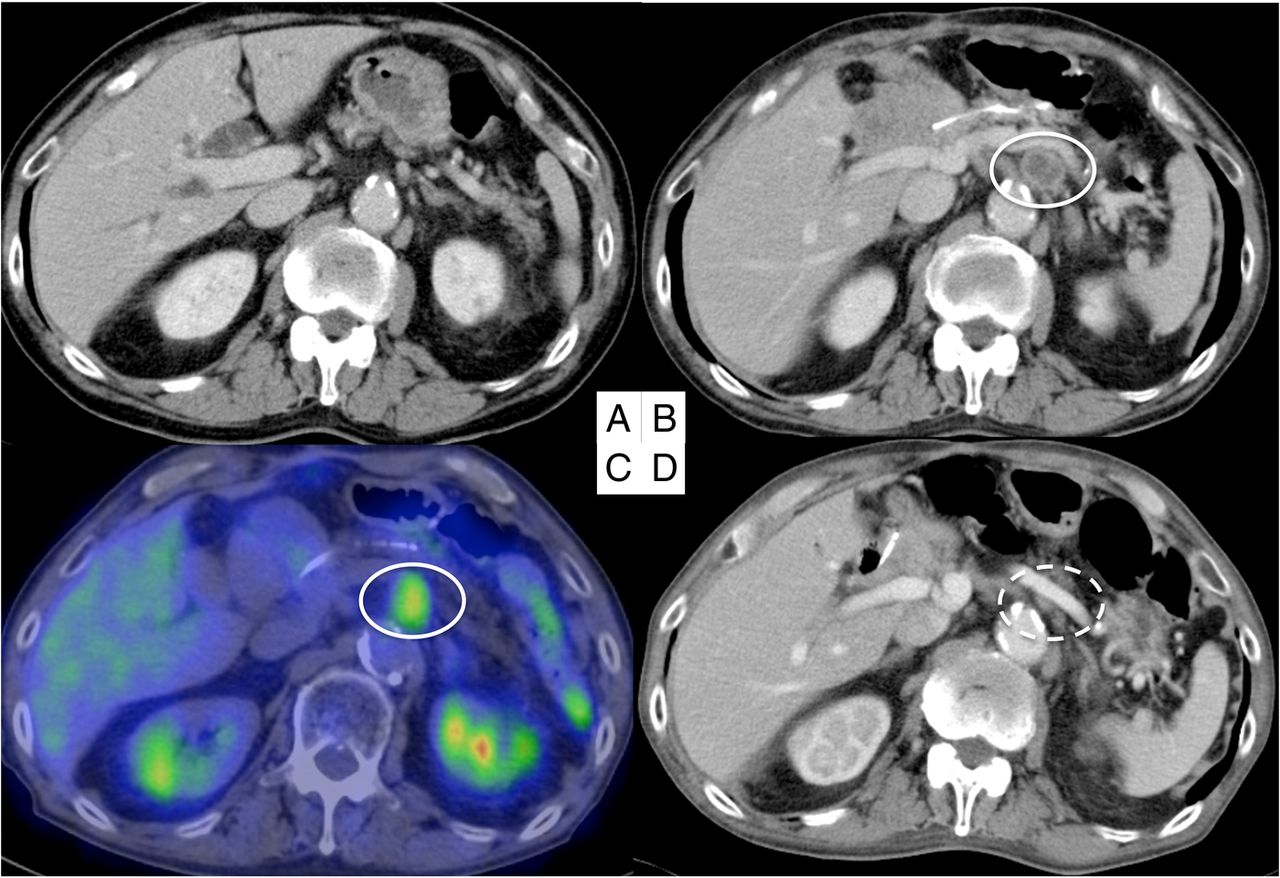
Six months after the operation, abdominal CT (figure 5A) and 18F-fluorodeoxyglucose positron emission tomography (figure 5B) were performed which revealed para-aortic lymph node recurrence. Chemotherapy with cisplatin (45 mg/m2 on day 8 every 5 weeks) and tegafur/gimeracil/oteracil (S-1; 100 mg/day for 21 days followed by 14 days of rest) was administered. After five courses of chemotherapy, abdominal CT was performed twice. The metastatic lymph node around the abdominal aorta disappeared, and the complete response was confirmed by imaging (figure 5C). The patient is alive without recurrence, 10 months after the first recurrence and chemotherapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Preoperative abdominal CT showed no metastasis around the abdominal aorta. (B and C) Abdominal CT and 18F-fluorodeoxyglucose positron emission tomography revealed the lymph node recurrence around the abdominal aorta (from the upper margin of the coeliac trunk to the lower margin of the left renal vein). (D) The metastatic lymph node around the abdominal aorta disappeared after chemotherapy.
Discussion
The biliary mucosa consists of a single layer of cylindrical epithelium without the existence of squamous cells. SCC of the bile duct is defined as ‘composed entirely of squamous cells with highly variable degrees of differentiation’ based on the fourth edition of WHO Classification of Tumours of the Digestive System.2 It is separated with adenosquamous cell carcinoma, which is adjacent or mixed with adenocarcinoma components and squamous cell components in the same lesion. SCCs of the bile duct are rare with an incidence of <1.4%.3 Between 1930 and 2016, there were only 14 cases describing SCC of the bile duct including the present case.1 ,4–15 Clinical analyses of these 14 cases of SCCs including our case are shown in table 1. The ratio of male to female incidence was ∼1:1. The average age was 64.5 years (range 24–86) and the median survival time after surgery was 12.0 months (range 3–32). The initial Union for International Cancer Control (UICC) staging was stage I in one case, stage II in three cases, stage III in two cases and stage IV in four cases. The initial staging was unknown in four cases; however, they tended to complicate synchronous or metachronous liver metastasis or peritoneal metastasis, suggesting advanced cancers. A radical resection was performed in seven cases;4 ,10 ,11 ,13–15 however, three cases had metachronus liver metastasis, one case had local recurrence and one case had metachronus lymph node metastasis. In the 13 cases which had metastasis, the percentage of metastasis was 38.5% in the liver, 15.4% in the N2 lymph nodes and 15.4% in the peritoneum.
Reported cases of squamous cell carcinoma of the extrahepatic bile duct
The potential mechanism of SCCs of the biliary tract is classified broadly into four theories as follows: (1) derivation from ectopic squamous epithelium, (2) derivation from undifferentiated basal cells, (3) transformation of adenocarcinoma to SCC and (4) derivation from metaplastic squamous epithelium of the glandular tissue.13 An experimental study of a murine model has shown that adenocarcinoma of the biliary tract may sometimes transform into adenosquamous carcinoma and ultimately to SCC.16 Mutou et al17 found that SCC proliferates two times faster than adenocarcinoma, suspecting adenosquamous carcinoma as the final stage of SCC. Therefore, transformation of the adenocarcinoma to SCC has been generally supported by cases of adenosquamous carcinoma. On the other hand, since Cabot1 proposed the theory of carcinogenesis from squamous metaplasia of the biliary mucosa caused by inflammatory irritation, derivation from metaplastic squamous epithelium of glandular tissue has been generally supported by cases of pure SCC. In the present case, SCC without adenocarcinoma components was shown in the serial sections from the entire area of the bile duct and in the metastatic lymph node. However, as the image of metaplastic changes such as dysplasia were not shown, the mechanism of the present case was difficult to explain.
Up to now, there is no worldwide criteria accepted for early bile duct cancer. The concept of early bile duct cancer is defined by the Japanese Society of Hepato-Biliary-Pancreatic Surgery,18 and the criterion is based on the depth of cancer invasion confined within the FM layer of the extrahepatic bile duct regardless of the possibility of lymph node metastasis. Therefore, the present case is defined as an early SCC of the bile duct due to the depth of tumour invasion, according to the Japanese staging system. On the contrary, UICC TNM Classification (seventh edition) does not define early stage of biliary tract cancer anywhere.19 Since the present case had regional lymph node metastasis, the case is recognised as having more advanced disease internationally. However, lymph node metastasis rarely occurs in tumours limited to the mucosa or FM layer because lymph ducts usually appear in the subserosa of the bile duct wall with nerve fibres and lymph nodes, causing lymphatic invasion, vascular invasion, perineural invasion and lymph node metastasis. Therefore, we had a question why lymph node metastasis occurred in the present case invading only the FM layer. Takahashi20 reported that there was a significant relationship between lymphatic invasion and perineural invasion in bile duct cancer. Furthermore, they reported that lymphatic invasion was seen ∼40% in FM cancers. Therefore, in the present case, we considered that the cancer cells separated from the primary lesion flowed and circulated inside the lymphatic channel of the FM layer, followed by engraftment and proliferation to the lymph node, and caused metastasis.
There was another question why recurrence occurred in the para-aortic lymph nodes. We hypothesised that there was a lymphatic drainage route between the para-aortic lymph node and the anterosuperior lymph node along the common hepatic artery, which was dissected during surgery. Ito et al21 reported that lymphatic drainage of the biliary tract is divided into two major pathways. (1) The cholecystoretropancreatic pathway, which has two routes, one running spirally and posteriorly from the anterior surface of the common bile duct to the right, and the other running almost straight down from the posterior surface of the common bile duct to reach the right side of the abdominal aorta nodes from the upper to lower margin of the left renal vein. (2) The cholecystocoeliac pathway is the route by which some of the lymphatics run to the left through the hepatoduodenal ligament to reach the coeliac nodes and left side of the abdominal aorta nodes from the upper to lower margin of the left renal vein. Taking these findings together, we considered that postoperative recurrence of the para-aortic lymph node (from the upper margin of the coeliac trunk to the lower margin of the left renal vein) was due to recurrence through the cholecystocoeliac pathway.
Surgical resection is the only curative treatment for bile duct cancer. Surgical indication depends on assessment of (1) patient's medical risk factors, (2) local tumour extension, and (3) distant metastasis such as N2 lymph nodes, lung, liver or peritoneal metastasis.22 Resectable distal bile duct cancer requires the removal of the pancreatic head, usually PD with extended bile duct resection. PD is a standard procedure that includes lymph node dissection and reconstruction of the stomach, the remaining pancreas and the bile duct. Pylorus-preserving pancreatoduodenectomy (PPPD) was introduced in order to reduce marginal ulceration and improve postoperative nutritional status after PD.23 Since delayed gastric emptying (DGE) had increased in PD and PPPD performed cases, SSPPD has been performed in Japan to try to maintain the pooling ability of the stomach and decrease the incidence of DGE.24 The present case underwent SSPPD to prevent the delay of oral food intake, hospital stay and the risk of aspiration pneumonia caused by inhaling materials due to DGE.
Chemotherapy and radiotherapy have been used in the reported cases of SCC of the bile duct for adjuvant chemotherapy or metastatic advanced cancer or postoperative recurrent cases. Although there is currently no evidence to support radiotherapy postoperatively or for unresectable bile duct cancers, radiation still has important palliative value, for example, for painful localisable metastasis or uncontrolled bleeding.25 In the previous presented cases, three cases were treated with radiotherapy and one case was treated with chemoradiotherapy. In those cases, radiation was used for palliative care in three cases and one case was used to prevent local recurrence. The authors intended to use radiotherapy since SCCs are generally more sensitive to radiation compared with adenocarcinomas. Clinical trials have shown that the standard chemotherapy for locally advanced or metastatic unresectable bile duct cancer (which is generally adenocarcinoma) is cisplatin plus gemcitabine.26 ,27 Yamana et al13 reported a case of SCC of the perihilar bile duct treated with chemotherapy (first line: 5-fluorouracil (5-FU) plus cisplatin (FP), second line: gemcitabine plus S-1) because of recurrence in the liver 6 months after surgery, who died 12 months after surgery. Goto et al15 reported a case of SCC of the perihilar bile duct treated with eight courses of gemcitabine as adjuvant chemotherapy, following with four courses (stopped due to progression of dementia) of gemcitabine because of local recurrence, who died 32 months after surgery. Other cases included regimens of cyclophosphamide plus doxorubicin plus methotrexate plus procarbazine,4 and one case had no description about the regimen.12 In these chemotherapy-treated cases, the present case was the only case showing complete response after recurrence.
S-1-based chemotherapy and the combination of S-1 and cisplatin has been used widely in Japan to treat several gastrointestinal malignancies. It is a combination of three pharmacological compounds, namely tegafur (a prodrug of 5-FU, which belongs in the group of antimetabolites), gimeracil (a potent dihydropyrimidine dehydrogenase inhibitor) and oteracil (an inhibitor of phosphorylation of 5-FU in the gastrointestinal tract).28 However, S-1 has not yet been included in the standard chemotherapy internationally. One reason for this is that the pharmacokinetics of tegafur is affected by polymorphisms in cytochrome P-450 2A6, and Western individuals are more likely to have higher 5-FU concentrations in the plasma compared with Japanese individuals.29 The standard chemotherapy for bile duct cancer is gemcitabine plus cisplatin. However, chemotherapy for SCC of the bile duct has not been established in the present state. So we used other cancer regimens originating from SCC such as oesophageal cancer and lung cancer as a reference. Chemotherapy of oesophageal cancers includes docetaxel plus cisplatin plus 5-FU therapy and FP therapy. The non-inferiority of S-1 plus cisplatin (SP) therapy compared with docetaxel plus cisplatin therapy is reported in the advanced non-small cell lung cancers.30 Taking these findings together, we selected SP therapy as the first-line treatment considering the regimen of SCCs of these SCC-originated cancers and the insurance adaptation in Japan of biliary tract cancers. Since the present case was the only case to represent complete response after recurrence, we considered regimens should be selected based on the origin of cancer histopathology findings.
As in the present case, SCC of the bile duct can develop recurrence due to metastasis in spite of curative resection. Therefore, a closed follow-up after radical resection should be considered concerning metastasis in the lymph nodes. Also, the curative effect of chemotherapy for resectable cases and unresectable cases are possible. Accumulation of future case reports will be needed to assess further treatment outcomes.
Learning points
After curative resection of the squamous cell carcinoma (SCC) of the bile duct, a closed follow-up is required concerning metastasis from the lymph node, although the depth of tumour invasion is shallow.
Although there is no standard chemotherapy for SCC of the bile duct, regimens should be selected based on histopathology findings of the cancer.
The treatment outcomes for SCC of the bile duct have not been well documented, and this case highlights the need for accumulation of future case reports in these patients.
References
Footnotes
Contributors RN drafted the manuscript. DHK was operator of the patient. DHK and MH revised the manuscript and TS has approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.