Article Text

Statistics from Altmetric.com
Description
A healthy man aged 32 years, with no notable family or medical history and no history of trauma, reported of sudden severe back pain on stretching and holding his breath while working at his desk. Apart from tachypnoea, his vital signs and physical examination were normal. A chest radiograph showed mediastinal widening (figure 1). Results of laboratory tests, including coagulation tests—prothrombin time, activated partial thromboplastin time and erythrocyte sedimentation rate—were all within normal limits. Contrast-enhanced CT revealed a mediastinal haematoma surrounding the descending aorta, with no aortic dissection or extravasation (figure 2). Contrast oesophagography detected no oesophageal rupture. Intercostal artery catheter angiography demonstrated no extravasation or aneurysm. Given his haemodynamic stability, conservative management was initiated. On day 2, repeat CT showed some haematoma absorption. One month postadmission, the haematoma had resolved.
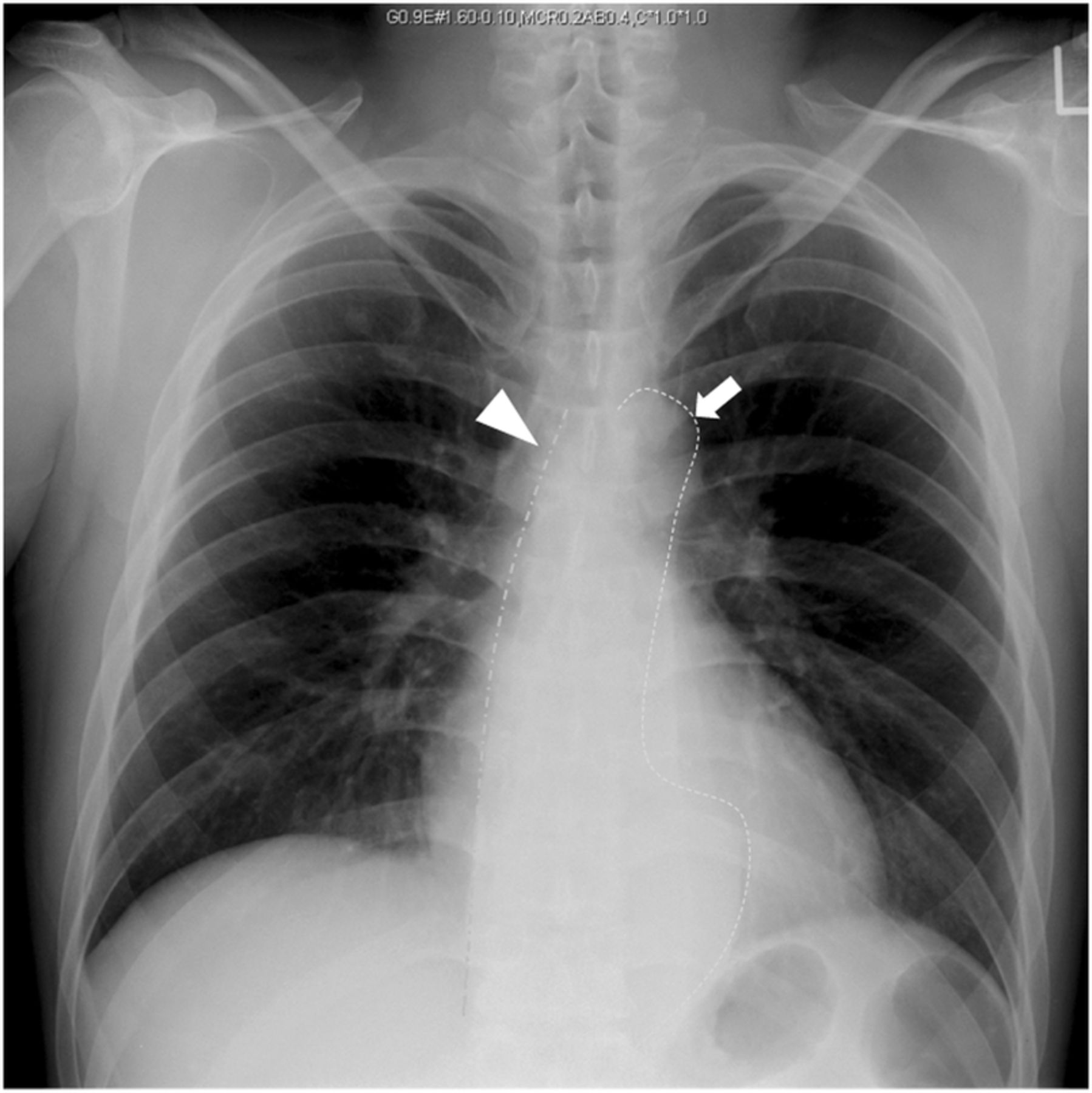
Chest X-ray showed widening of the right paraspinal line (arrowhead) and para-aortic line (arrow).

{kind=link}
{kind=link}
Sagittal contrast-enhanced CT showed the mediastinal haematoma surrounding the descending aorta (arrows).
Although rare, a spontaneous mediastinal haematoma may result from mediastinal small-vessel injury following a sudden intrathoracic pressure increase.1 It presents with chest pain and dyspnoea.2 Determining the bleeding origin is vital. Minimally invasive port-access thoracoscopy can be used in haemodynamically stable, low-risk patients. Alternatively, such patients can be managed conservatively, with serial imaging to assess haematoma resolution.3
Learning points
Physicians should consider a spontaneous mediastinal haematoma when finding mediastinal widening on chest radiography.
Determining the bleeding origin is vital.
In haemodynamically stable in young people with no risk, spontaneous mediastinal haematoma can be managed conservatively, with serial follow-up imaging to assess for resolution.
Footnotes
Contributors YC, YI and KS contributed to patient management. YC drafted the initial manuscript. RI critically reviewed manuscript. All authors contributed to writing the manuscript. All the authors have provided written consent for publication.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.