Article Text

Statistics from Altmetric.com
Description
A 7-year-old previously healthy girl presented with 1-day history of headache and unsteady gait. Neurological examination revealed intranuclear ophthalmoplegia, vertical nystagmus and ataxic gait. CT scan showed hyperdense haemorrhagic lesion in the fourth ventricle (figure 1) and MRI further demonstrated a large focus of haemorrhage in the posterior pons and surrounding oedema with two small foci of enhancement along the anterior margin of the mass (figure 2). Craniotomy was performed for evacuation of the haemorrhage and biopsies were taken from the area. Neuropathology demonstrated a hypercellular glial tumour with pleomorphic nuclei and haemorrhage consistent with a high-grade glioma (figure 3). Molecular sequencing of the tumour showed mutations in p53, PDGFRa, PI3K, ASXL1 and H3F3A. The patient died 5 months after diagnosis due to disease progression.

Sagittal CT image demonstrating hyperdense haemorrhagic lesion in the fourth ventricle.
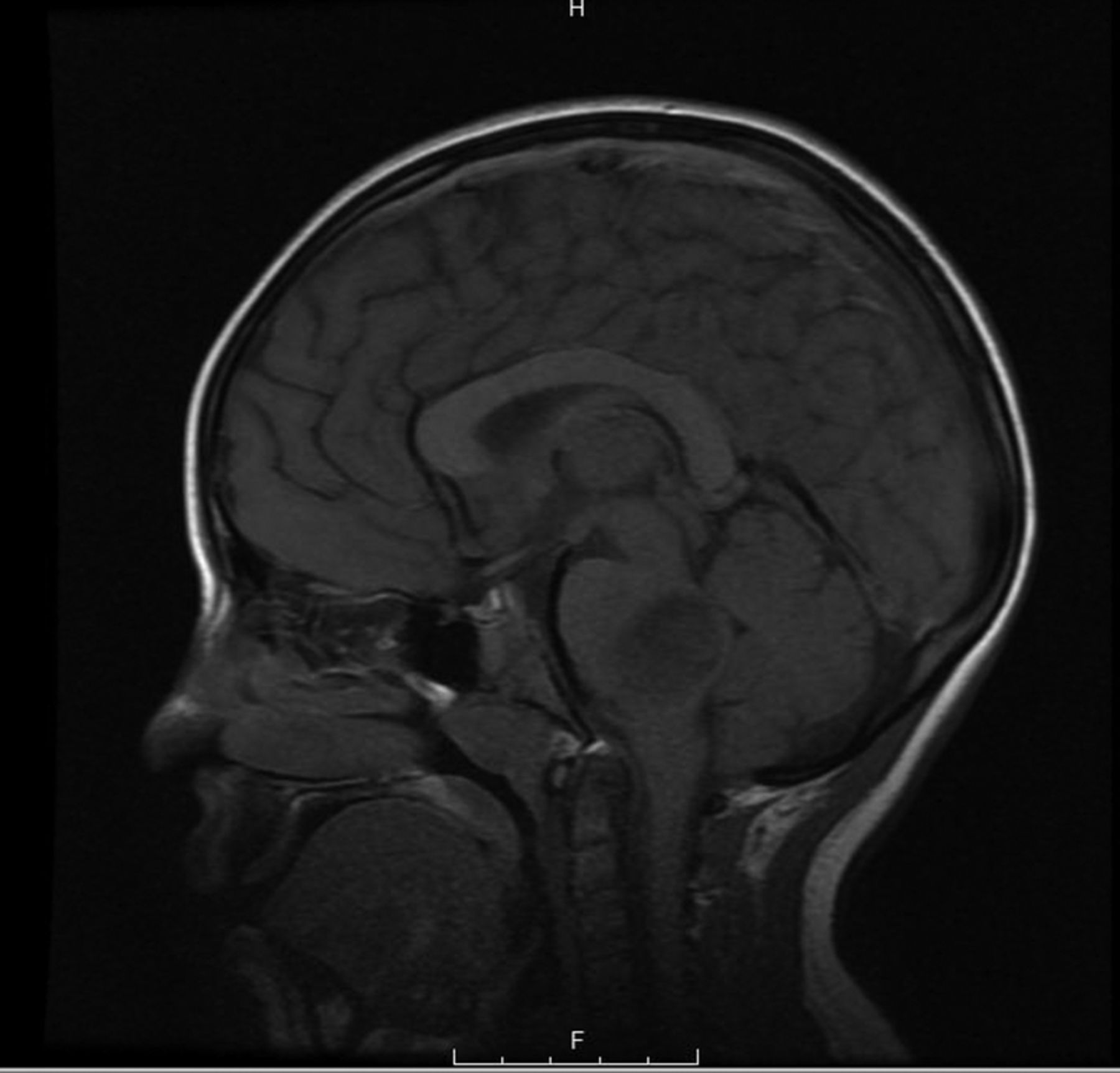
Sagittal T1 weighted image with contrast reveals large hypointense focus of haemorrhage in the posterior pons.

{kind=link}
{kind=link}
{kind=link}
H&E stain reveals hypercellular glial tumour with pleomorphic nuclei and haemorrhage consistent with a high-grade glioma (×40).
The patient's acute presentation of brainstem findings in conjunction with a haemorrhagic brainstem lesion is more commonly seen with aetiology of vascular origin, making this a unique presentation of a high-grade brainstem tumour. The differential diagnosis of brainstem lesions in children includes neoplastic, vascular, infectious and postinfectious causes1 ,2 This case highlights that it is important to include high-grade glioma in the differential of acute brainstem haemorrhage and the essential role of biopsy in establishing the diagnosis.
Learning points
Gliomas may be indistinguishable from ruptured cavernomas on CT imaging and should be considered in the differential diagnosis of acute brainstem haemorrhage.
Brainstem biopsy may be warranted in selected cases of acute brainstem haemorrhage to establish a diagnosis by an experienced neurosurgeon.
Footnotes
Twitter Follow Yasmin Aghajan at @yaghajan
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.