Article Text

Statistics from Altmetric.com
Description
A 30-year-old woman presented to the orthopaedics outpatient department with low back pain (LBP) for 4 weeks, not relieved on medications. She had no known comorbidities. On examination, there was movement restriction of the lower spine and focal right posterior lumbar tenderness. Blood routines showed raised acute inflammatory markers. Imaging work-up included a routine frontal radiograph of the lumbar spine which showed a lumbosacral transition vertebra with enlarged right transverse process (figure 1). Sacroilliac joints appeared normal. Plain MRI of the lumbar spine was performed which revealed lumbosacral transitional vertebra (LSTV) with enlarged transverse process articulating with the sacral ala bilaterally forming diarthroidal joint (Castellvi type IIb) and the subchondral bone of this joint showed T2 short τ inversion recovery hyperintense signals and hypointense signals on T1-weighted images, which was suggestive of marrow oedema. The intervening cartilage was also hyperintense. There were no signal abnormalities on the left side. Rest of the lumbar spine was normal. These features were suggestive of inflammatory changes occurring in an underlying pseudoarthrosis between the right transverse process of L5 and right sacral ala (figures 2–⇓4). Thus, a diagnosis of Bertolotti’s syndrome (BS) was made. Correlative plain multidetector CT scan of the lumbar spine was performed to demonstrate subtle osseous alterations at the site of pseudoarthrosis, which revealed a lumbosacral transitional vertebra (Castellvi type IIb) and a pseudoarthrosis between the right transverse process of L5 vertebra and the right sacral ala with minimal marginal spurring and reactive bone sclerosis (figures 5 and 6). The patient was managed with anti-inflammatory medications and percutaneous steroid injections, and she was symptom-free at discharge.

Frontal radiograph of the lumbar spine showing a lumbosacral transition vertebra with enlarged right transverse process (arrow). Sacroilliac joints appeared normal.
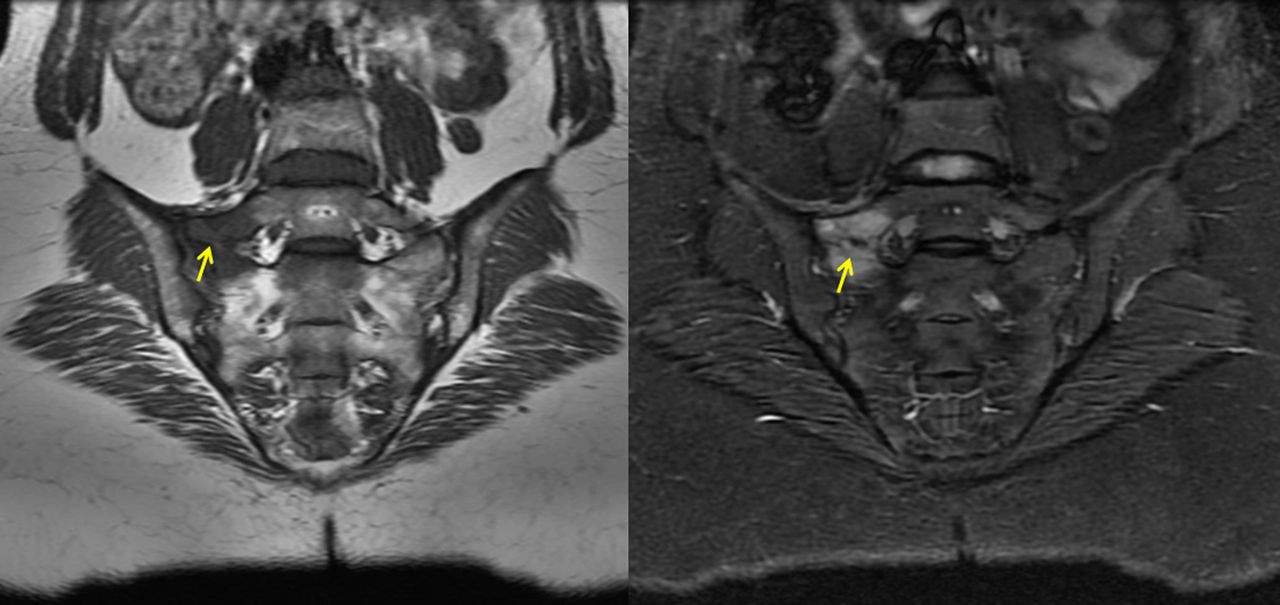
Oblique coronal corresponding T1-weighted (left) and T2-weighted (right) images of the sacrum and lower lumbar vertebra showing an inflammatory pseudoarthrosis (arrow) between the right transverse process of L5 vertebra and the right sacral ala.
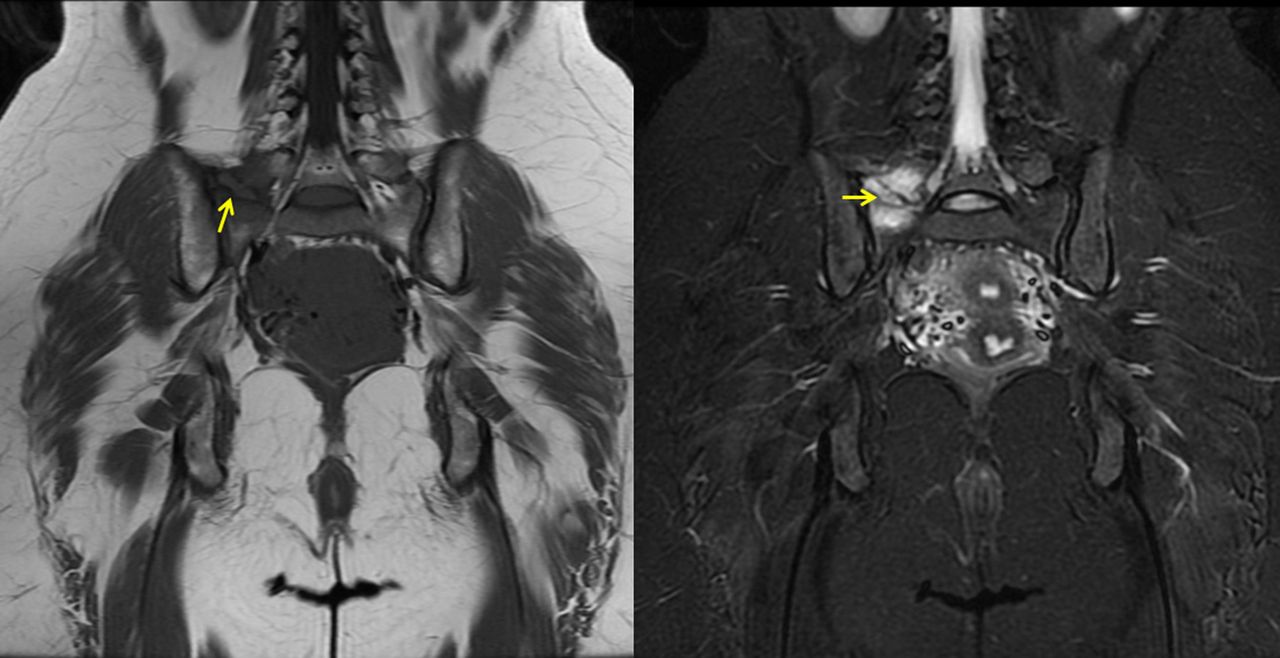
Oblique coronal corresponding T1-weighted (left) and T2-weighted (right) images of the sacral ala and the lower lumbar vertebra showing an inflammatory pseudoarthrosis (arrow) between the right transverse process of L5 vertebra and the right sacral ala.

Sagittal T2-weighted MRI of the lumbar spine showing normal disc and vertebral body signals.

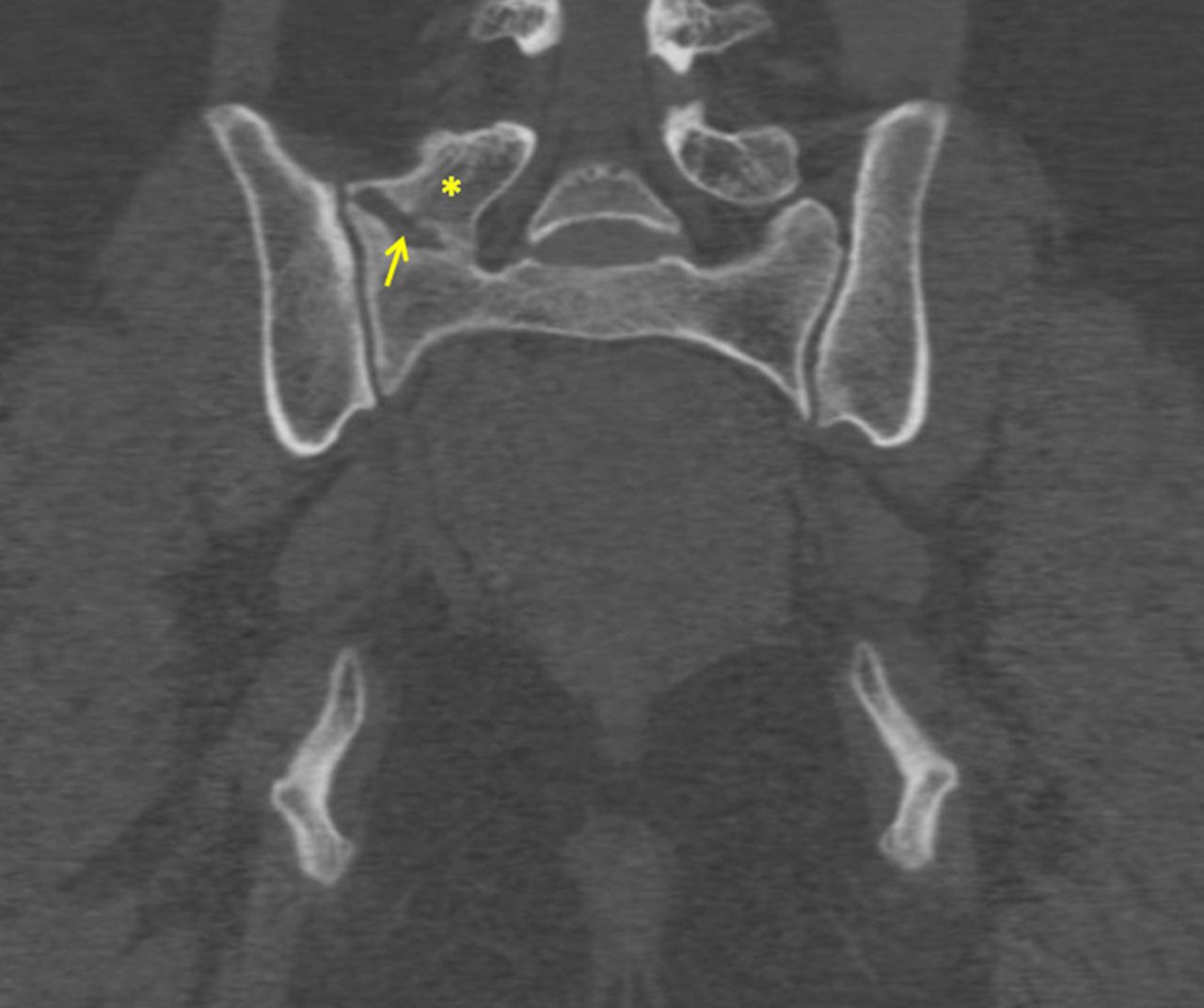
Coronal reformatted multidetector CT image of the sacrum and lower lumbar vertebra showing a pseudoarthrosis (arrow) between the right transverse process of L5 vertebra (asterisk) and the right sacral ala with marginal spurring and bone sclerosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Volume rendered CT image showing the pseudoarthrosis (arrow) between the right transverse process of L5 vertebra (asterisk) and the right sacral ala.
BS is characterised by the presence of a fifth lumbar (L5) vertebra anatomic variation with a large transverse process that forms a pseudoarthrosis or a bony fusion with the sacral basis or iliac crest, which then proceeds to arthritic changes at the site of pseudoarthrosis resulting in chronic/persistent LBP.1 It is an important cause of LBP in young patients, affecting upto 8% of the general population and 18.5% in individuals <30 years of age, although asymptomatic LSTV is prevalent in about 13% of the general population.2 Physical examination is non-specific, and shows mild to moderate tenderness at the lower back and range of motion of the spine may be limited and painful. The diagnosis of BS is based on imaging with clinical correlation.
Plain radiographs of the lumbosacral spine showing the presence of an enlarged transverse process of the L5 vertebrae that forms a joint/pseudoarticulation with the sacrum or the iliac bone suggests BS. CT will reveal marginal spurring, hypertrophy and reactive bone sclerosis. MRI is useful in revealing bone oedema around the inflamed pseudoarthrosis. Bone scans (nuclear scintigraphy) will reveal hypermetabolic areas as foci with isotope avidity.2
Standard AP radiographs demonstrate 76–84% accuracy for LSTV detection and mid-sagittal T2-weighted MRI predicts the presence of an LSTV with 80% sensitivity and 80% specificity. However, Ferguson radiographs (AP radiographs of the lumbosacral spine angled cranially at 30°) have slightly higher sensitivity than standard AP radiographs in diagnosing LSTV.3
Castellvi reported an imaging classification system for LSTV.4 Type I is an enlarged L5 transverse process, not clinically significant. Type II is the formation of a unilateral or bilateral diarthroidal joint between the enlarged transverse process and the sacrum. Type III is a unilateral or bilateral solid fusion and type IV is a mixed variant with a pseudarthrosis on one side.4
BS is essentially LBP in the presence of LSTV, therefore it is a spectrum. Among 4636 patients from the Osteoarthritis Initiative cohort, 3.9% of the patients without an LSTV reported LBP, 46% of patients with type I and 40% of patients with type III LSTV reported LBP. About 73% of patients with type II and 66% of patients with type IV LSTV reported LBP. These figures suggest that type 1 and type III LSTV may be protective anomalies relative to type II and type IV LSTV.5
Various treatment approaches are available which include percutaneous injection of anaesthetic medications and steroids, radiofrequency ablation of the anomalous diarthroidal joint, surgical fusion of the pseudarthrosis and osteotomy of the enlarged transverse process.6 ,7
Learning points
Bertolotti's syndrome (BS) is an important cause of low back pain in young patients with a reported incidence of 18.5% in individuals <30 years of age.
BS is characterised by the presence of a fifth lumbar (L5) vertebra anatomic variation with a large transverse process that forms a pseudoarthrosis or a bony fusion with the sacral basis or iliac crest, which then proceeds to arthritic changes at the site of pseudoarthrosis resulting in chronic/persistent low back pain.
Footnotes
Twitter Follow Sankar Neelakantan at @drsankar23
Contributors SN developed and conceived the idea of the case report. KS wrote the manuscript. RA edited the manuscript. BP approved the final version of the manuscript to be published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.