Article Text

Summary
Most ovarian inguinal hernias occur in children and are frequently associated with congenital genitalia defects. The authors present the case of a multiparous 89-year-old woman, without any genitalia defect, who was brought to the emergency department with an irreducible inguinal hernia. The patient was proposed for emergency surgery during which we encountered an ovary and a fallopian tube inside the hernial sac. An oophorosalpingectomy and a Lichtenstein procedure were carried out and the postoperative period was uneventful. This case shows that, even though it is rare, a hernial sac may contain almost any intra-abdominal organ, including those least frequent such as the appendix, an ovary or the fallopian tubes.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Hernias are a common problem in general surgery and about 75% of them occur in the inguinal region.1
An indirect inguinal hernia is the most common type of hernia, irrespective of the gender, and strangulation is its most dreadful complication, occurring in 1–3% of the cases, especially in the extremes of age.1
However, every once in a while, surgeons are surprised by the intraoperatory findings when performing a common procedure such as an inguinal hernia repair.
Case presentation
An 89-year-old woman presented to the emergency department with lower abdominal pain and a lump in her inguinal left region, since that morning. She had no symptom of bowel movements changes or fever.
The patient had recently been discharged from the internal medicine ward after a urinary tract infection and a perianal abscess treated after a 1-week antibiotic course.
She also suffered from chronic renal disease, chronic anaemia, high-blood pressure, cerebral vascular disease (with left hemiparesis after an ischaemic vascular accident) and dyslipidaemia.
Physical examination revealed a calm, awaked but disoriented patient. She was slightly dehydrated, haemodynamically well and afebrile. Her abdomen was diffusely painful, with rebound tenderness, especially in the lower quadrants. In the left inguinal region, a painful tense mass, of nearly 5 cm was documented. No inflammatory signs were visible and no external genitalia anomalies were found. Laboratory results were within normal ranges.
An incarcerated inguinal/femoral hernia was the initial hypothesis and so a pelvic ultrasound (US) was requested.
Investigations
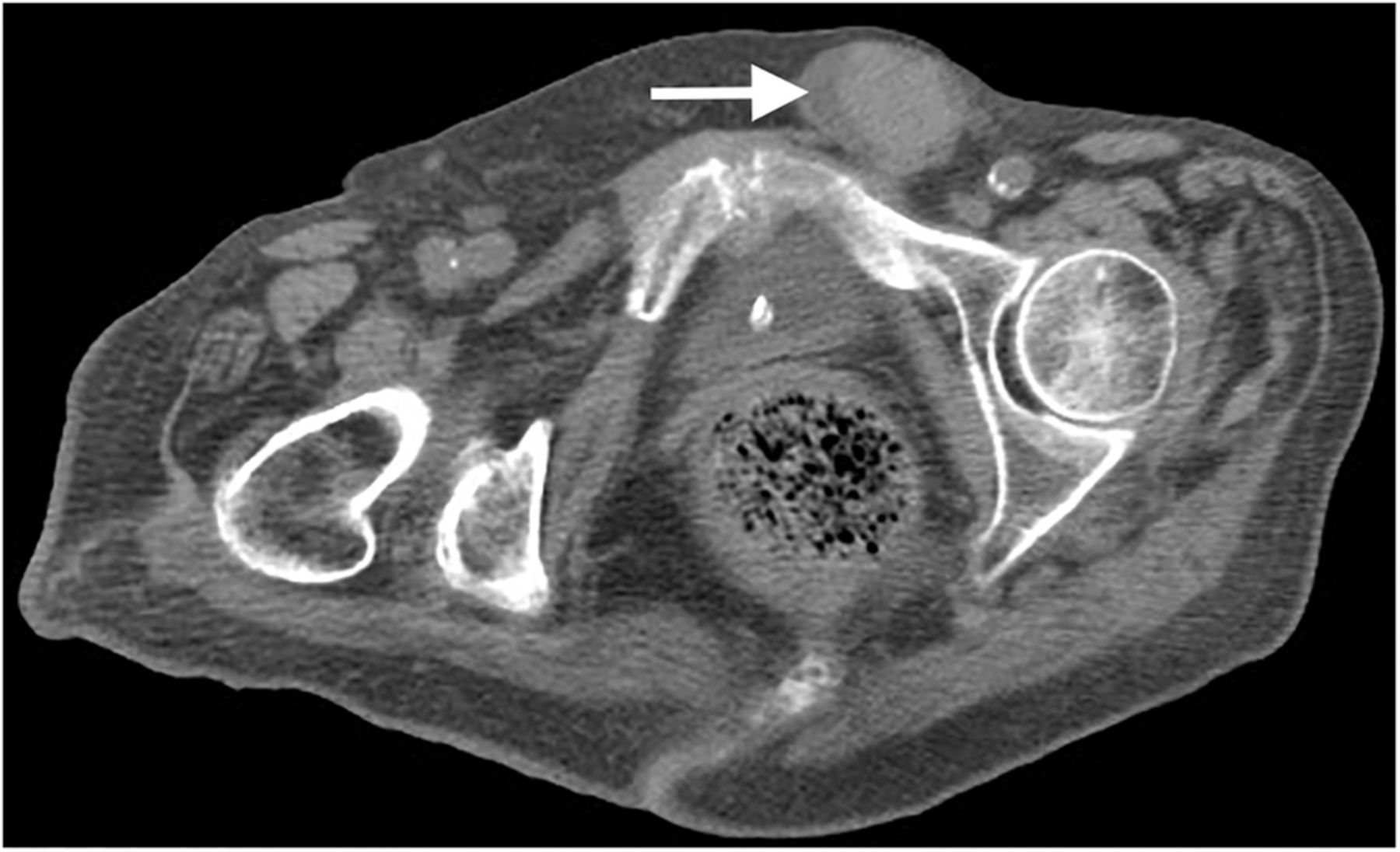
The attending radiologist performed an US scan and complemented it with a pelvic CT scan (figures 1⇓–3). On the left femoral duct, a well-defined, fine-walled, non-pure cystic formation was identified; admitting the continuity with the intestinal segment, the possibility of an incarcerated femoral hernia was considered. The same formation also appeared to be in continuity with the round ligament, suggesting the presence of canal of Nuck cyst.

Pelvic ultrasound scan.

Transverse section of pelvic CT scan. White arrow showing a ‘fine-walled, non-pure cystic formation’, hernial sac.

Coronal section of pelvic CT scan. White arrow showing a ‘fine-walled, non-pure cystic formation’, hernial sac.
Treatment
The patient was proposed for emergency surgery, accepted by the next of kin who signed the informed consent form.
Under regional anaesthesia (subarachnoid block), the authors performed an open inguinal hernia approach and found a hernial sac containing the left ovary and fallopian tube. A left oophorosalpingectomy and a Lichtenstein procedure—with a polypropylene mesh—were carried out without complications (figures 4⇓–6).

Left inguinal hernia (preoperatory).
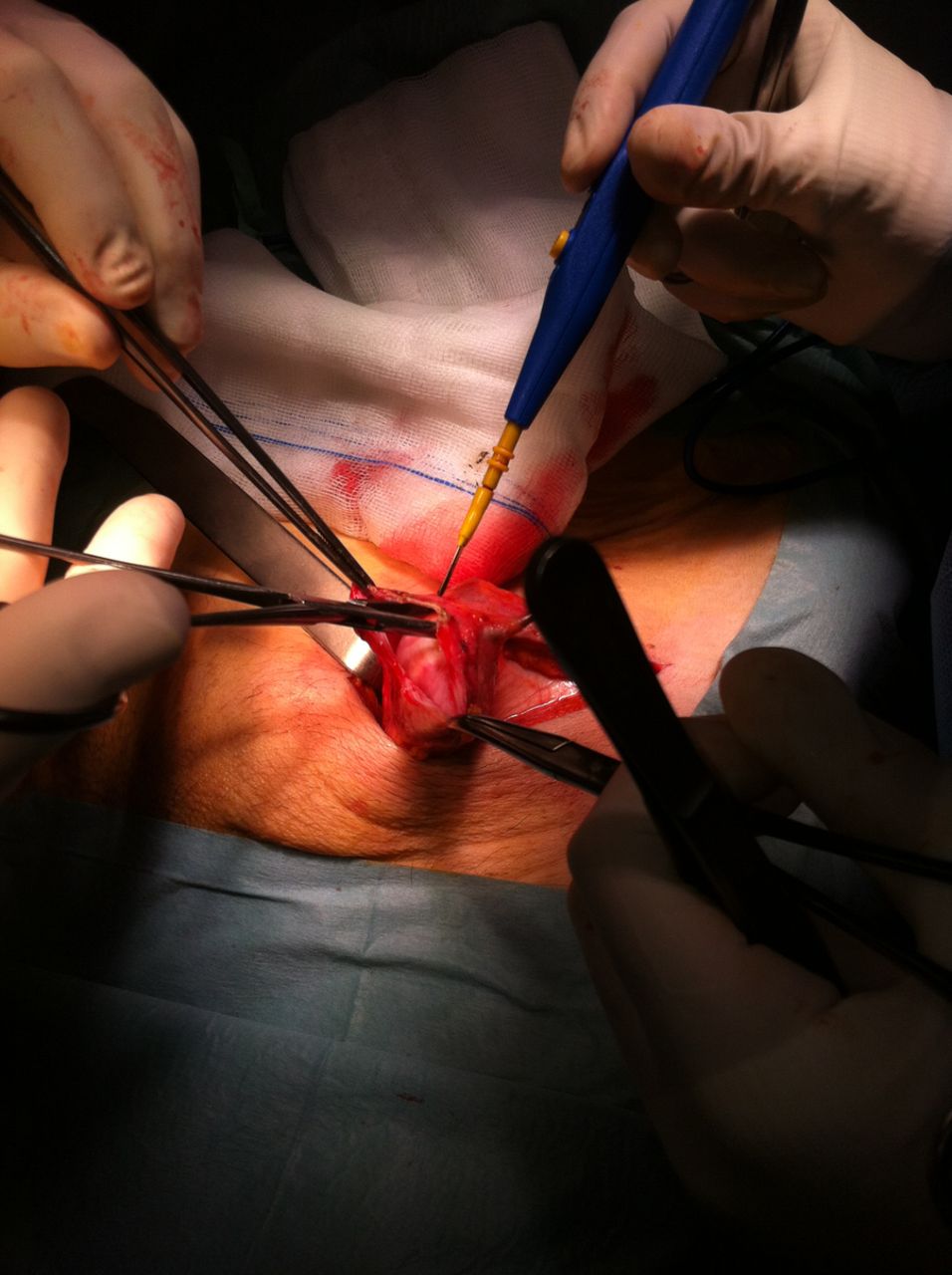
Opening of the hernial sac.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left ovary inside the inguinal hernial sac.
Outcome and follow-up
The patient was discharged 5 days after surgery, and referred to the outpatient clinic.
The anatomopathological examination revealed an ovarian fibroma (3.2×3.2×1.7 cm) and a fallopian tube (5.5×0.5 cm) without pathological findings.
Discussion
It is often said that any intra-abdominal viscera can be found inside a hernial sac and in nearly 3% of those cases female adnexa are encountered.2–4
Unlike men, female inguinal canal contains only the round ligament and vessels that run to the labia majora, providing a path to the development of inguinal hernias.
The majority of those hernias occur in paediatric ages and are usually associated with congenital anomalies of the genitalia.3
In premenopausal women, a rapid diagnosis and the prompt correction is crucial in order to save the adnexa from torsion and infarction and, therefore, ensure fertility.5
In postmenopausal women it has been hypothesised that the progressive weakness of the ligaments of the adnexa may add to the process of herniation. Furthermore, as these tissues have hormonal receptors, they are under the influence of several hormonal stimuli during a woman's life, from embryogenesis to parity, and even to the effects of systemic disease in intra-abdominal pressure.3
Our patient underwent two types of imaging diagnosis (US and CT), and yet the diagnosis was only confirmed intraoperatively. This case comes as a reminder that attention must be at highest when performing surgical dissection.
It is known, that ovarian herniation may also be associated with anomalies of the ovary and fallopian tube; for that reason, we decided to perform an oophorosalpingectomy and requested an anatomopathological examination.
Although our patient was a multiparous woman, with several comorbidities, there were no pathological findings in the resected specimen.
As it is our usual practice in elective inguinal hernia repair, a polypropylene mesh was used to close the hernial defect.
After discharge, the patient's follow-up was carried out in the outpatient clinic, during several months without evidence of recurrence. She passed a way due to pneumonia, 6 months after surgery.
Learning points
We describe a rare finding inside an inguinal hernial sac, especially in an adult, multiparous woman.
When elaborating the differential diagnosis of an irreducible groin mass, one must consider the possibility of compromised organs in order to avoid severe complications.
Even though we are equipped with technological innovations that enable us to achieve imagiological diagnosis before surgery, we also know that some of these examinations are operator dependent. Therefore, a high level of suspicion and adequate patient information must be provided to the attending radiologist in order to improve preoperatory diagnostic accuracy.
Nevertheless, some of these cases will only be correctly identified through careful surgical dissection.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous