Article Text

Statistics from Altmetric.com
Description
A 20-year-old man was assessed for a genital ulcer that developed after an episode of orchiepididymitis. On the initial physical examination, a grey longitudinal melanonychia was found on the left index finger, measuring 4.5 mm in diameter, with mild subungual hyperkeratosis (figure 1A, B). A longitudinal nail biopsy was performed (figure 2A) and the histological analysis revealed a pigmented squamous cell carcinoma (SCC) (figure 2B). Total nail apparatus excision with placement of a full-thickness graft harvested from the retroauricular area was performed with no recurrence after 1-year follow-up.

(A) Clinical photograph showing a longitudinal grey melanonychia of 4.5 mm diameter. (B) Dermoscopic view of the tumour. A curved grey melanonychia with small darker globules can be observed.
{kind=link}
{kind=link}
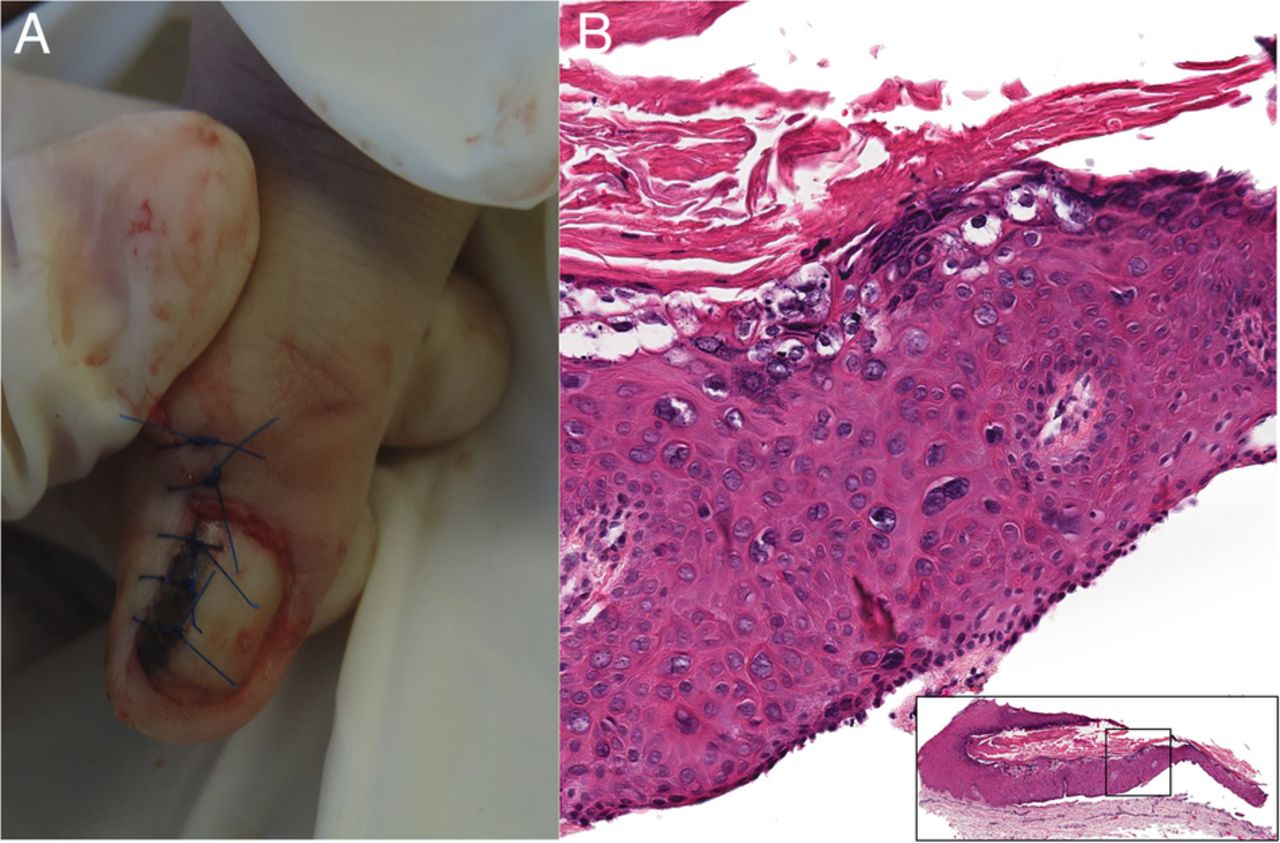
(A) Longitudinal nail biopsy was performed. (B) Histopatological sections show full-thickness atypia of the nail bed.
Pigmented SCC of the nail unit is an uncommon tumour. A <10% of these tumours present as longitudinal melanonychia. It occurs more commonly after the fifth decade of life,1 and only a few reports on young patients have been previously reported. Men are affected up to twofold more than women are.2
Several risk factors have been associated with the development of subungual SCC: ultraviolet radiation exposure, repeated trauma, pesticides or arsenic exposure and human papilloma virus infection.2
Lack of awareness of this tumour leads to a delay in its diagnosis. Prompt nail biopsies of new onset or persistent melanonychias should be encouraged to exclude malignant tumours such as melanoma or pigmented SCC.2
Given the rarity of this tumour, treatment guidelines have not been established. Wide surgical excision is the preferred treatment, with a relapse rate of <5%. Mohs micrographic surgery is advised for limited lateral tumours and once the tumour has invaded bone tissue, amputation should be performed.1 ,2
Learning points
Ten per cent of squamous cell carcinoma (SCC) of the nail apparatus cases present as longitudinal melanonychia.
The differential diagnosis of a longitudinal melanonychia should include benign and malignant lesions: nevi, onychomycosis, traumatic melanonychia, verruca vulgaris, melanoma and SCC.
An early diagnosis of subungual SCC leads to more conservative surgeries, with a better functional and cosmetic outcome.
Footnotes
Twitter Follow Michelle Gatica- Torres at @kalygatica
Contributors MG-T and LA-G contributed to patient's follow-up and manuscript writing. JMR-M contributed to patient's surgery and follow-up, as well as to manuscript editing. JD-C contributed to manuscript editing and reference review.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.