Article Text

Statistics from Altmetric.com
Description
Herpes simplex virus (HSV) is the most common non-epidemic and sporadic cause of viral meningoencephalitis with an incidence of approximately 1–3 cases per million.1 Ninety five per cent of fatal adult cases are a result of type 1 HSV (HSV-1) and typically follow latent viral reactivation in the trigeminal ganglion in immunocompetent patients.1 MRI is regarded as being the most sensitive radiological investigation, with changes usually visible within 2–3 days of onset of symptoms.1 Traditionally on MRI, Herpes simplex encephalitis (HSE) exhibits bilateral asymmetrical involvement of the limbic system, including the medial temporal lobes, insular cortices and inferolateral frontal lobes and cingulate gyri.1 Sparing of the basal ganglia is a key feature, which also helps in differentiating from middle cerebral artery infarction on diffusion-weighted imaging (DWI). Atypical patterns, if seen, usually affect the younger population with involvement of the cerebral hemispheres and rarely, the midbrain and pons.1
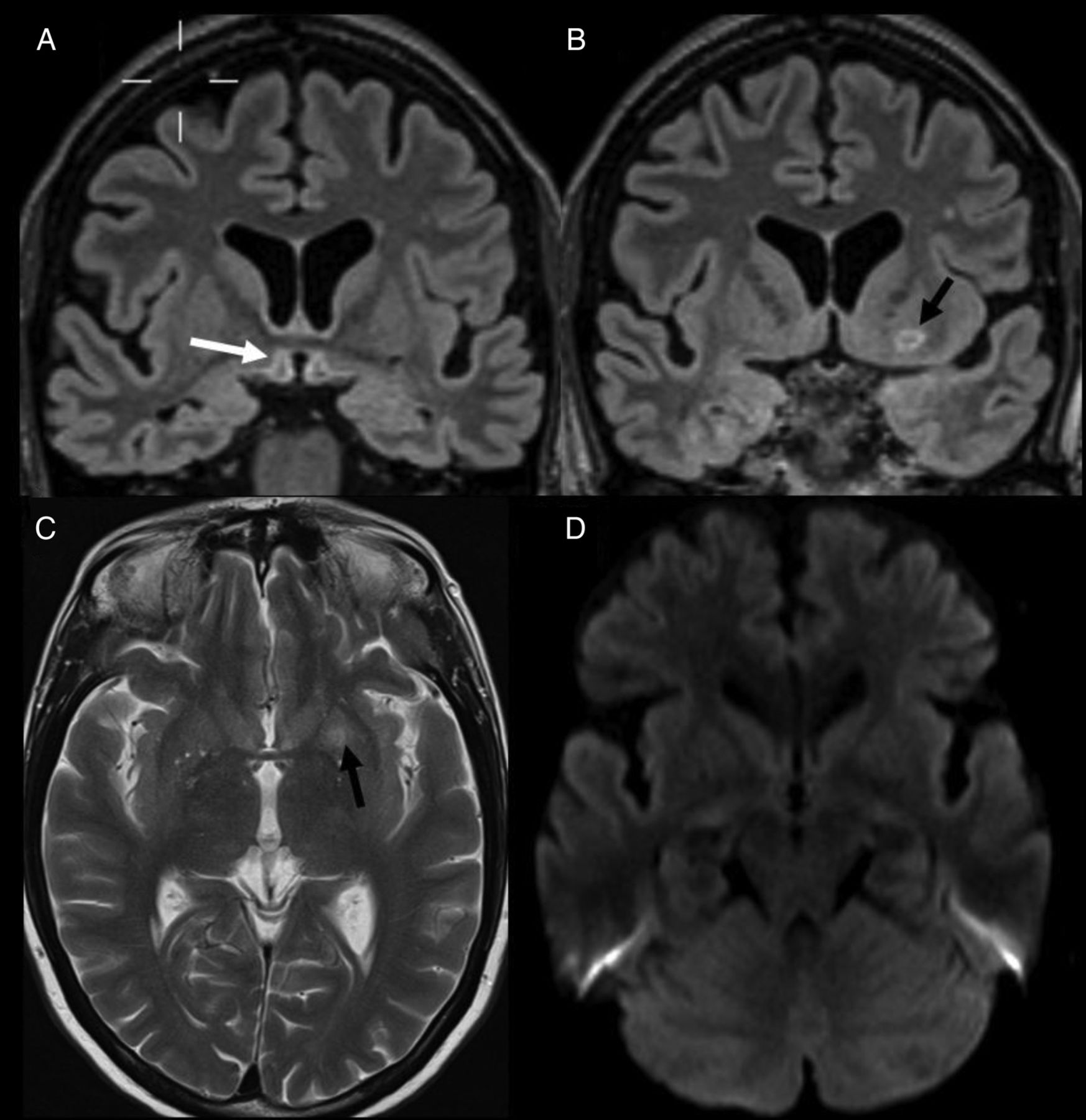
We present serial brain imaging of a 52-year-old woman who presented to the acute medical unit with a week's history of lethargy, intermittent headaches and an episode of syncope prior to admission. Over the course of the subsequent 24 h, she developed acute confusion and became hypotensive, hypothermic and bradycardic. CT of the brain was not of any diagnostic value. MRI, however, demonstrated grossly abnormal signal change in the hypothalamic region at the floor of the third ventricle and optic chasm and optic tracts on both sides, with partial involvement of the inferior aspect of the left putamen (figure 1A–D). DWI showed a lesser degree of symmetrical restricted diffusion involving the paramedian structures (figure 1E, F). There was no significant enhancement with intravenous contrast (figure 1G, H). The imaging findings were considered unusual and atypical for usually seen acute neurological conditions, although the possibility of Wernicke encephalopathy was raised.

Initial MRI findings. T2 axial (A), fluid-attenuated inversion recovery coronal (B–D) showing hypothalamic and floor of third ventricle involvement (white arrows), putamen involvement (black arrows), optic chiasm involvement (white broken arrow). Diffusion-weighted imaging and apparent diffusion coefficient (C and D) showing smaller areas of restricted diffusion (white arrows). T1 sagittal precontrast (G) and postcontrast (H) showing no enhancement.
Lumbar puncture for cerebrospinal fluid (CSF) examination revealed 94×106/L white cell count (100% lymphocytes) with elevated CSF protein (3042 mg/L) and normal CSF glucose (4.2 mmol/L). Viral PCR on CSF was positive for HSV-1. The MRI scan was reviewed and on literature review, no similar example of HSE was found with similar MRI findings; a possibility of false-positive PCR was also raised, however, sensitivity and specificity of PCR testing for HSV is accepted to exceed 95%.2 Surprisingly, several clinical manifestations of HSE, such as cold sores, were also not present. However, there was no history of alcoholism or gastrointestinal (GI) surgery to have predisposed the patient to Wernicke's encephalopathy.
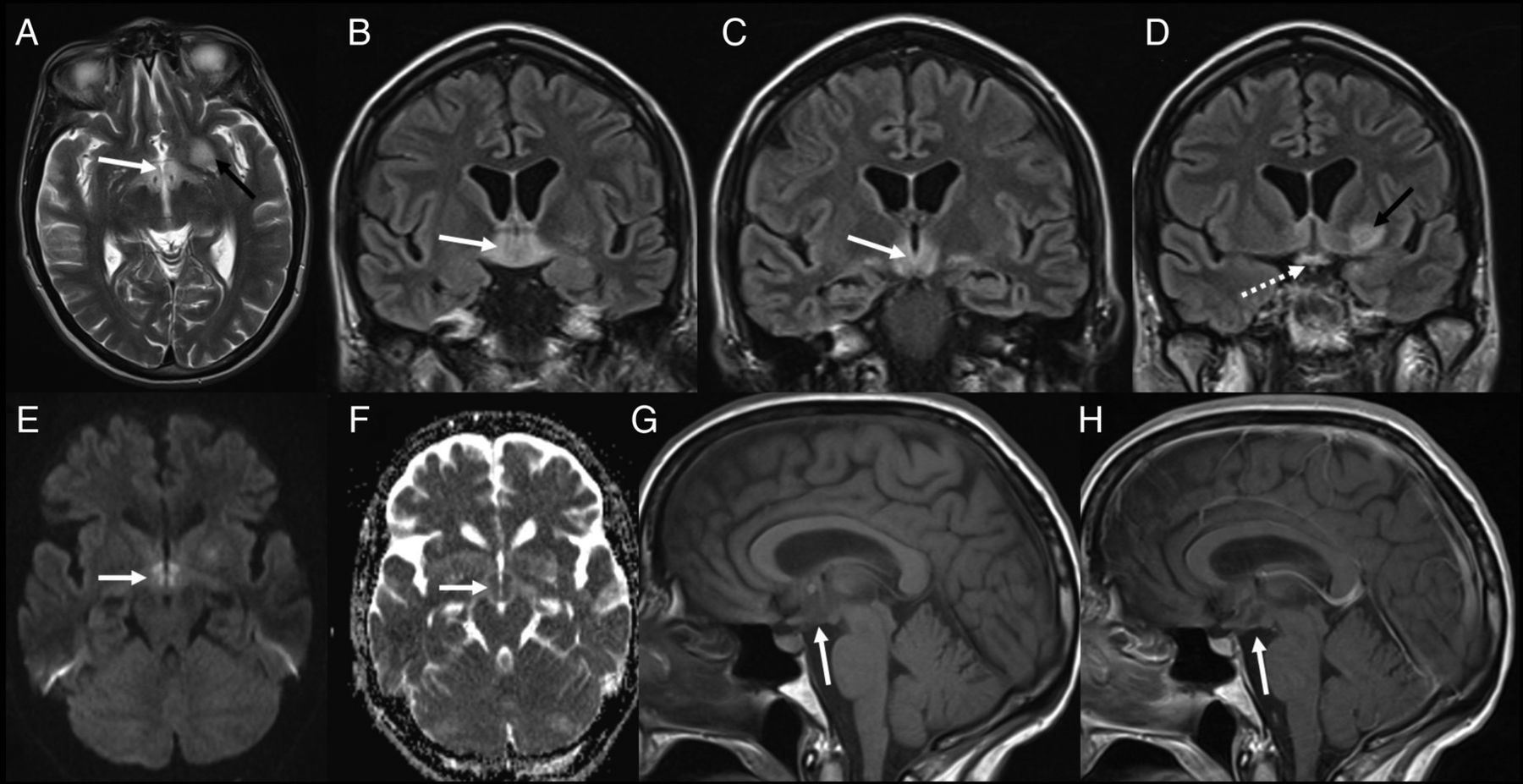
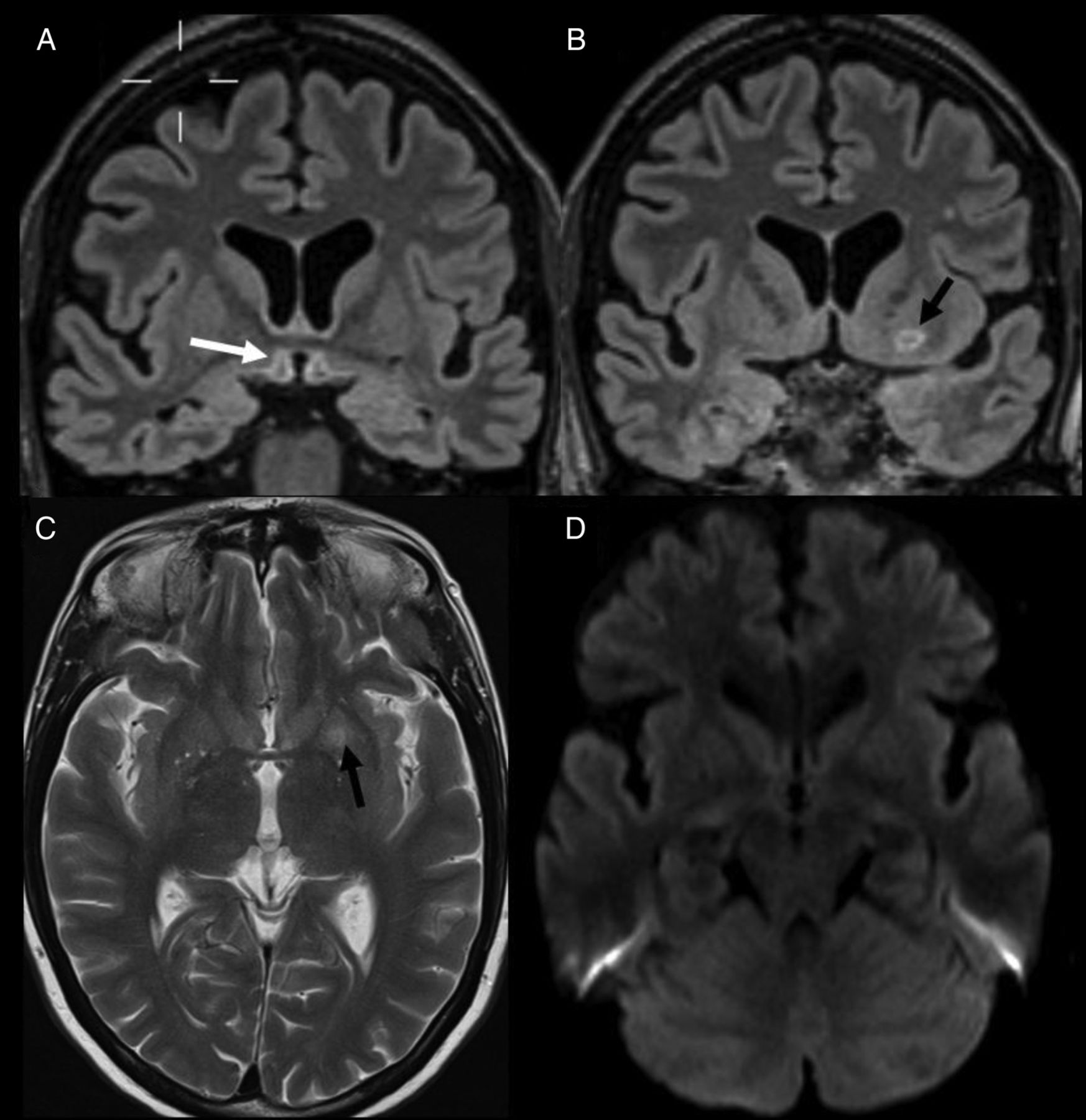
Patient was treated with antiviral therapy, although due to unusual MRI findings, intravenous thiamine was also given. Patient's hypothermia improved over the next few days and the patient subsequently developed fever. Clinical improvement followed over the course of 2 weeks. Two follow-up MRIs were performed over the next 8 weeks (figures 2 and 3), that revealed an overall improvement in signal appearances in the hypothalamus, the left lentiform nucleus and optic chasm and optic tracts, but residual changes in the form of subtle high signal persisted. Notably, the usual MRI features of HSE never developed. Four weeks after discontinuing antiviral medication, the patient developed unilateral acute retinal necrosis (ARN). The strong association of ARN with herpesviruses3 prompted further treatment with antiviral and immunosuppressive therapies. HSV-1 infection was subsequently again proven through positive vitreous PCR. Despite treatment, the present case resulted in cognitive impairment and the patient was subsequently transferred to a neurorehabilitation unit.

Follow-up MRI at 4 weeks. Fluid-attenuated inversion recovery coronal (A and B) and T2 axial (C) showing improvement in hypothalamic signal (white arrow) and putemen (black arrow). Diffusion-weighted imaging (D) showing reduced signal abnormality (white arrow).
{kind=link}
{kind=link}
{kind=link}
Follow-up MRI at 8 weeks. Fluid-attenuated inversion recovery coronal (A and B) and T2 axial (C) showing further evolution of hypothalamic signal with subtle cavitation (white arrow) and putemen (black arrow). Diffusion-weighted imaging (D) showing resolution of signal abnormality (white arrow).
MRI is the modality of choice in imaging assessment of the hypothalamus.4 Lesions affecting this region can be broadly classified into the following: neoplastic (primary and secondary), developmental, inflammatory/granulomatous diseases and lesions arising from the adjacent brain parenchyma.4 Wernicke encephalopathy is an acute neurological condition resulting from a dietary Vitamin B1 (thiamine) deficiency and characteristically symmetrically involves the mamillary bodies, dorsomedial thalami, tectal plate, periaqueductal area and the grey matter around the third and fourth ventricle.5 ,6 It usually happens in a background of alcoholism or GI resection.
We have presented an unusual case of proven HSE, where the typical MRI findings were absent. There was hypothalamic involvement with hypothermia, which, to the best of our knowledge, has not been described before along with putamen involvement which is also rare. HSE should be included as a differential diagnosis when evaluating acute hypothalamic lesions on MRI.
Learning points
Herpes simplex encephalitis (HSE) can rarely involve hypothalamus and present as hypothermia. It should be included in the differential of hypothalamic lesions.
HSE may also involve putamen, although it is rare.
HSE can occur with absence of typical findings in temporal lobes and insula.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.