Article Text

Statistics from Altmetric.com
Description
A 42-year-old woman attended the dermatology outpatient department (OPD), with a 2–3 year history of multiple firm flesh-coloured papules localised to her cheeks, periauricular and auricular area (figures 1 and 2). These lesions developed when the patient was in her late 30s. They were asymptomatic. She also had multiple fibroepithelial polyps (skin tags). She had a family history of similar skin lesions (2 sisters and her father). Her medical history was significant for mild hidradenitis suppurativa.

Multiple firm flesh-coloured papules—right post-auricular area.

Multiple similar lesions affecting nasal bridge and ala.
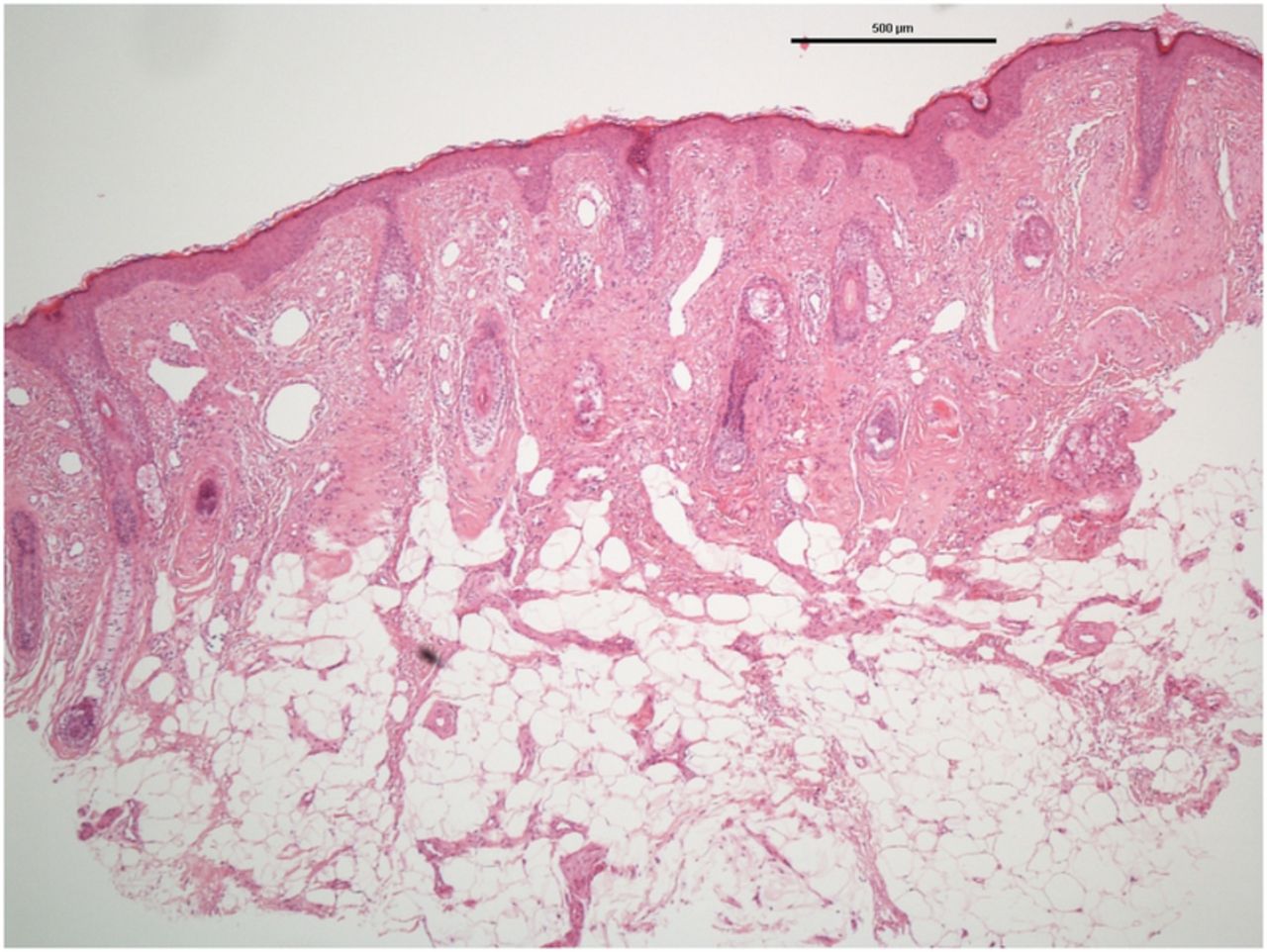
A punch biopsy of lesional skin was performed—histology showed focal increase in perivascular dermal connective tissue, in keeping with an angiofibroma (figures 3 and 4). Genetic testing confirmed a heterozygous variant in the folliculin (FLCN) gene, consistent with a diagnosis of Birt-Hogg-Dubé syndrome.

H&E stain—angiofibroma, left earlobe.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
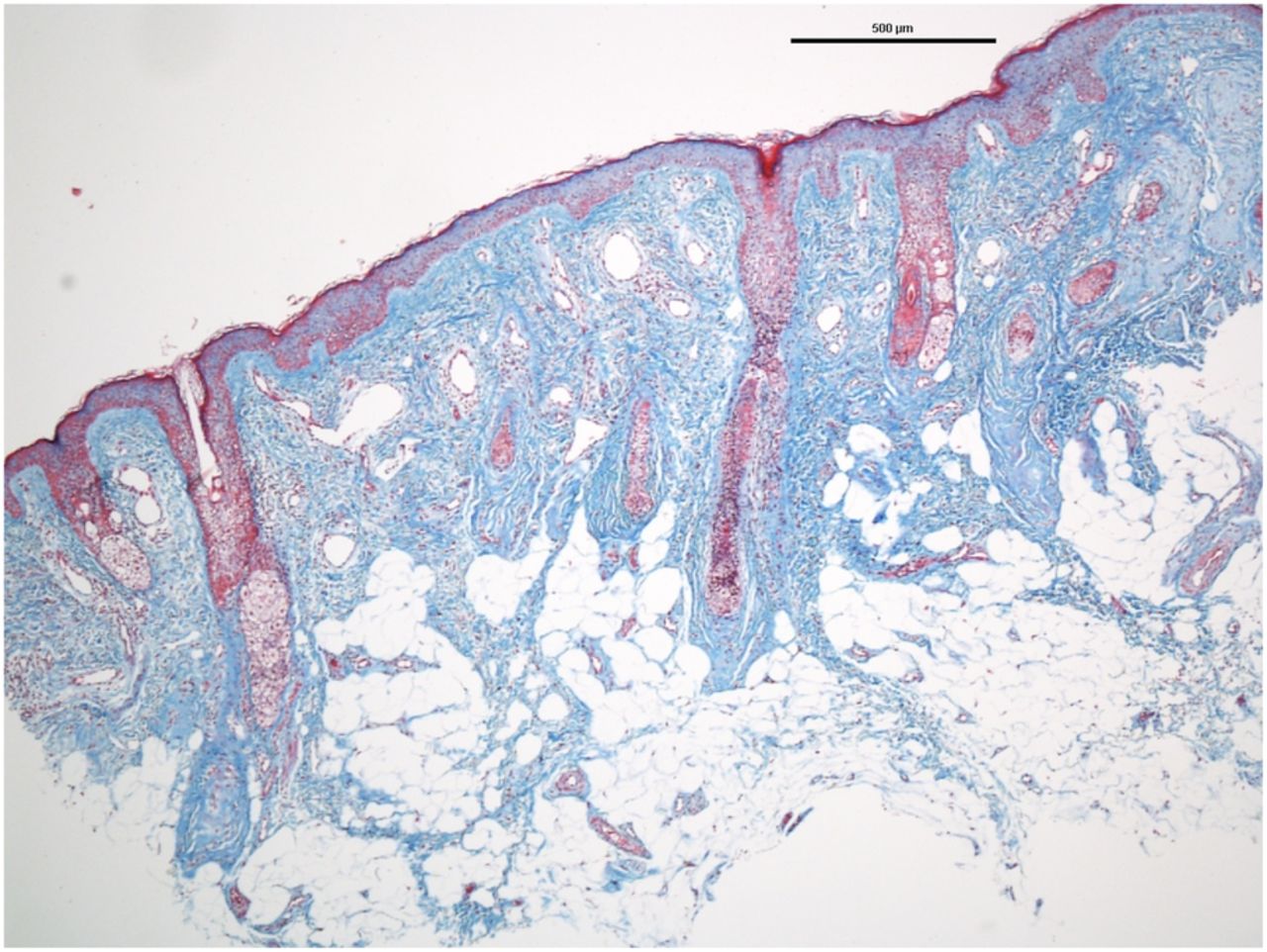
Masson's trichrome—highlighting fibrosis in an angiofibroma, left earlobe.
Birt-Hogg-Dubé syndrome is an autosomal-dominant condition. It has characteristic cutaneous findings, including fibrofolliculomas, angiofibromas, fibroepithelial polyps and trichodiscomas. Extra cutaneous findings include pulmonary cysts, spontaneous pneumothorax and renal cancer.1 Management is focused on early diagnosis and treatment of renal cancer.1 The FLCN gene, located on the short arm of chromosome 17 (17p11.2), is responsible for this syndrome.2 It codes for the protein folliculin, thought to be an oncogene suppressor protein. It has also been linked to the mammalian target of rapamycin signalling pathway, a serine/threonine protein kinase that regulates cell growth, proliferation and survival.3
Following diagnosis of Birt-Hogg-Dubé syndrome, our patient had a renal ultrasound and thorax/abdomen CT to assess for pulmonary or renal disease. These revealed a benign renal cyst with no evidence of pulmonary cysts. She will require long-term follow-up and screening for renal carcinoma.
Learning points
Multiple angiofibromata are associated with several genetic conditions including tuberous sclerosis, multiple endocrine neoplasia type 1 (MEN1) and Birt-Hogg-Dubé syndrome.
Skin examination can help detect patients who may be at risk of certain malignancies and who may therefore benefit from regular cancer screening.
Diagnosing a genetic condition has implications for both the patient and all family members.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.