Article Text

Statistics from Altmetric.com
Description
A 23-year-old Japanese man experienced sudden acute pain from the throat to the chest while cooking. On admission, his vital signs were stable and he had no remarkable medical or family history. He denied fever, recent illness, cough, vomiting, dyspnoea, dysphonia, drug abuse, alcohol use, smoking and trauma. He had never taken any medication and had never used recreational drugs. Physical examination indicated a pneumoderma on the patient's neck, but no precordial crunching sounds on auscultation. Bedside echocardiography indicated poor visualisation, regardless of the presence of bilateral lung sliding. Plain chest radiography showed air dissecting along the descending aorta and intersecting with a band extending along the medial left hemidiaphragm (figure 1). CT showed emphysema from the neck to mediastinum without pneumothorax (figures 2 and 3), indicating spontaneous pneumomediastinum (SPM). The patient had an uneventful recovery and was discharged on day 6.

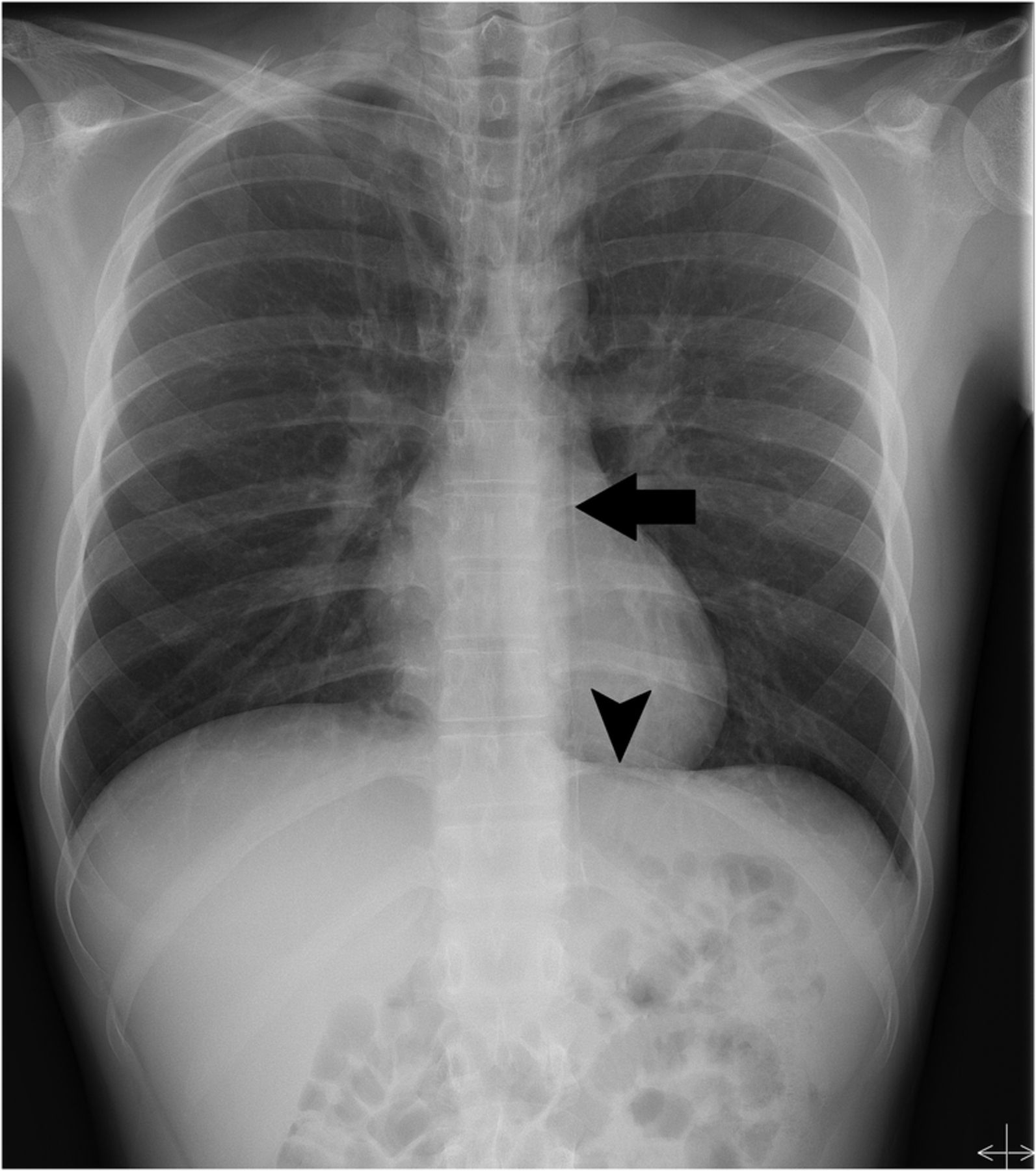
Chest radiograph showing substernal gas anterior to the aorta (deep cervical emphysema, arrow), as well as gas between the diaphragm and the pericardium, which renders the superior margin of the left hemidiaphragm visible (continuous diaphragm sign, arrowhead).

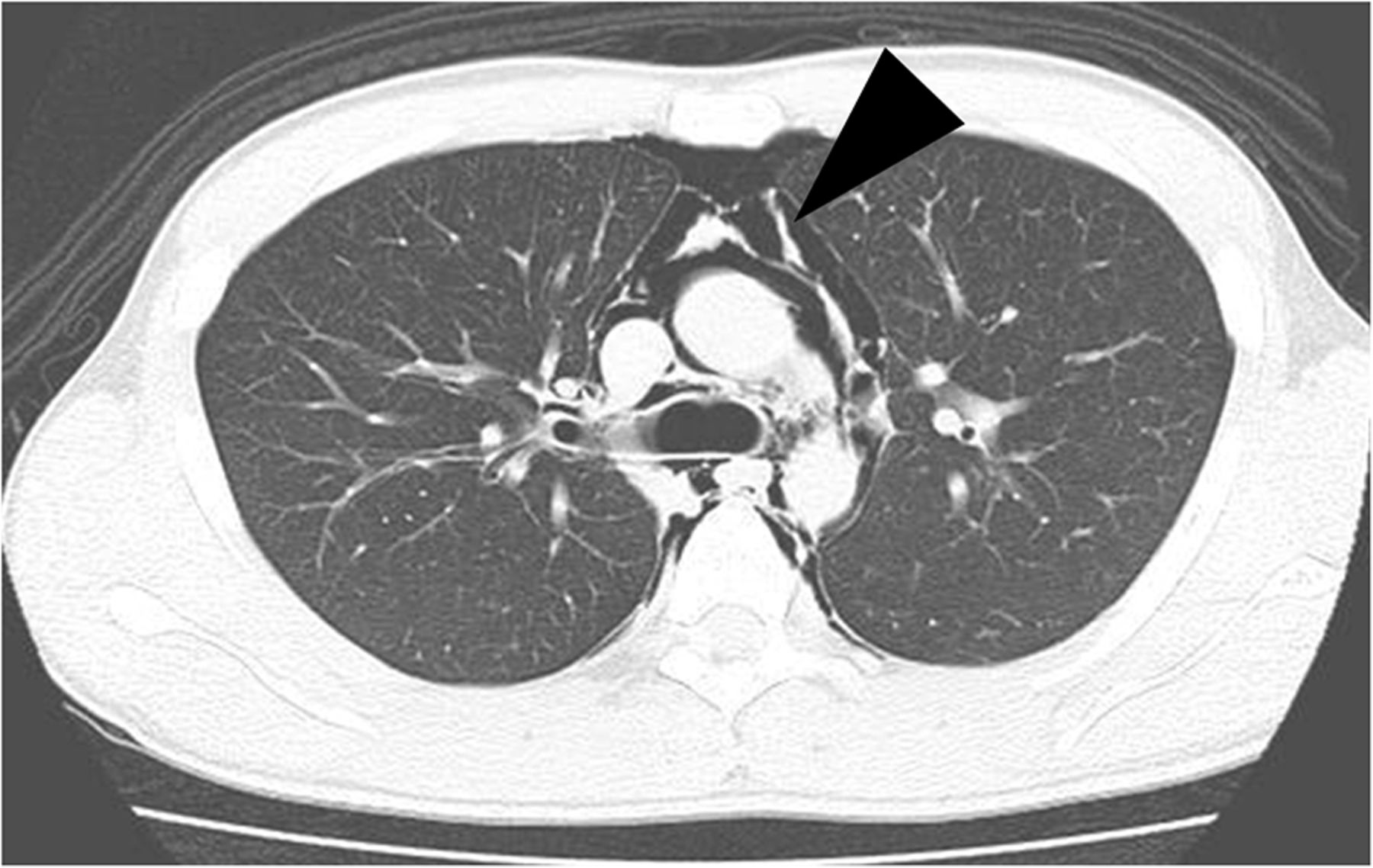
Chest CT showing emphysema around the patient's trachea (arrows) and oesophagus.
{kind=link}
{kind=link}
{kind=link}
Chest CT showing emphysema around the paravertebral area (arrowheads), without pleural fluid on the left.
SPM is a rare condition; the most frequent symptoms include chest and neck pain in young men. It mainly develops due to alveoli rupture, as a result of increased internal pressure caused by severe coughing or breath holding.1 Subcutaneous emphysema is detected on physical examination in approximately 58% patients, but crunching sounds with heart sounds (Hamman’s sign) are noted in only 18% of patients.2 Pneumomediastinum is most commonly diagnosed using chest radiography, but the causes of secondary pneumomediastinum (gas-producing organisms/oesophageal rupture) should be excluded. Ultrasonography enables a quicker evaluation of SPM in clinical practice. SPM is mainly treated with observation, but may be fatal if complications such as infection or tension pneumothorax develop.3 Hence, when young patients present with acute chest pain and poor echocardiography findings, idiopathic mediastinal emphysema should be considered in the differential diagnosis.
Learning points
When young patients present with acute chest pain and poor echocardiography findings, physicians should consider idiopathic mediastinal emphysema.
Spontaneous pneumomediastinum is a rare condition, but may be fatal if complications such as infection or tension pneumothorax develop.
Footnotes
Contributors All the authors contributed to patient management. KK and RI drafted the initial manuscript. All the authors contributed to writing the manuscript and have provided written consent for publication.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.