Article Text

Statistics from Altmetric.com
Description
A 68-year-old woman presented with worsening sound-induced vertigo (Tullio phenomenon) and left-sided hearing loss. Weber's test lateralised to the affected ear and audiography confirmed mild conductive hearing loss. Neurological assessment was remarkable for torsional/vertical noise and vibration-induced nystagmus. The patient demonstrated low threshold cervical vestibular-evoked myogenic potential responses, and superior semicircular canal dehiscence was suspected. Otoscopy, tympanography and stapedial reflexes were normal bilaterally.
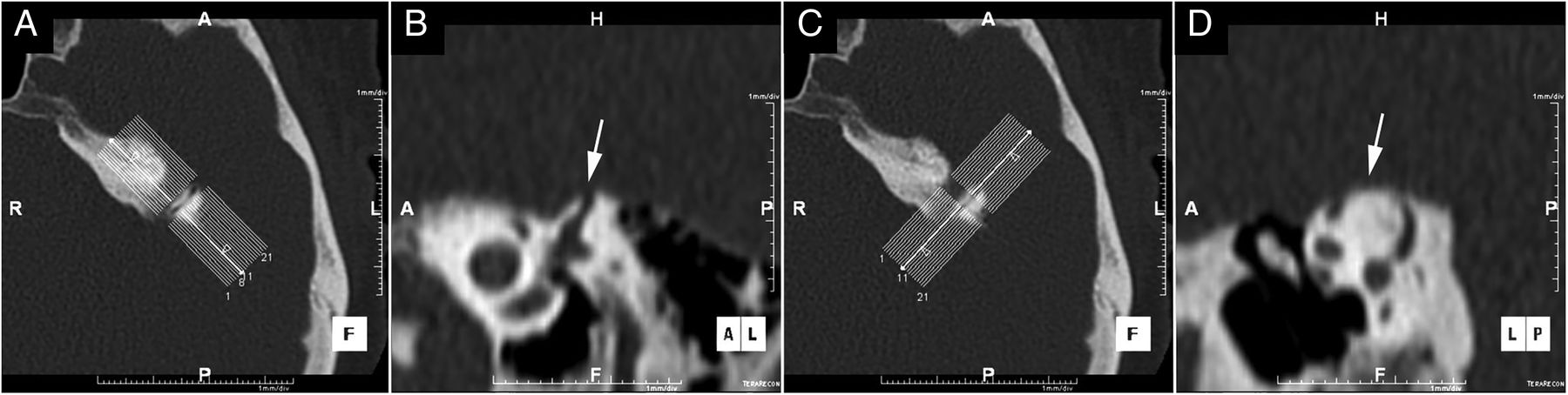
High-resolution CT of the temporal bones was performed, which demonstrated a bony defect in the apex of the superior semicircular canal (figure 1).

{kind=link}
High-resolution CT of the temporal bones reconstructed in the Stenvers (A and B) and Pöschl (C and D) planes demonstrating a bony defect in the apex of the superior semicircular canal (B and D, arrows).
The thin osseous plate covering the semicircular canal may be breached by trauma or erosive processes resulting in corruption of the hydraulic purity of the perilymph. Surgical repair of the defect with fascia or canal resurfacing is effective and provides long-term symptom relief.
While in the majority of cases superior semicircular canal dehiscence (SSCD) is the main pathology in patients with the Tullio phenomenon, other causes include an enlarged vestibular aqueduct and perilymphatic fistulae.1 The pathophysiology of this phenomenon is thought to be that the dehiscence of the superior circular canal creates a mobile window in the labyrinth allowing the transmission of low frequency sound waves. This in turn causes movement of the endolymph inside the canal, triggering the vestibular signs and symptoms exhibited in these patients.2
Learning points
The majority of cases of Tullio phenomenon are due to superior semicircular canal dehiscence.
While the Tullio phenomenon is an unusual combination of signs and symptoms, a clinical history and focused examination are usually sufficient to make the diagnosis.
Footnotes
Twitter Follow Richard Pullicino at @Rikardu
Contributors Both RP and RG contributed in the formatting of the images and the description of the case.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.