Article Text

Statistics from Altmetric.com
Description
A dysgerminoma is a very rare and malignant tumour originating from the ovarian primordial germ cells. Germ cell tumours account for 2.6% of all ovarian malignant tumours and about 70% of cases of ovarian cancer in the early decades of life, and are found very rarely thereafter.1 ,2
The authors describe the case of a previous healthy 22-year-old woman, nulligravida, with a history of right ovarian dysgerminoma FIGO (International Federation of Gynaecology and Obstetrics) stage IC (conservative fertility surgery with full staging—right salpingo-oophorectomy, conservation of the uterus and left adnexae with positive peritoneal lavage cytology for malignant cells, without residual neoplasia and no nodal metastases, and negative left ovary and peritoneal biopsies—and three cycles of adjuvant chemotherapy with the bleomycin/etoposide/cisplatin scheme, had been performed). Five months after surgical staging and chemotherapy treatment, the patient was admitted in the emergency ward, because of pain in the left iliac fossa, with a bulky pelvic mass bulging on the left vaginal fornix in the gynaecological examination. Pelvic ultrasound showed a suspected 100.4×77.2 mm left cystic adnexal mass with multiple and small septa (figure 1), confirmed by pelvic CT (figure 2) and MRI (figure 3). With supposed pelvic recurrence, the patient underwent laparotomy and a large lymphocoele was found and drained. The left ovary had a normal macroscopic appearance.

Ultrasound findings—complex cystic left adnexal mass with large transverse diameter of 77.2 mm causing mass effect on the bladder (represented on the left top of the image). There were no suspicious findings on Doppler.
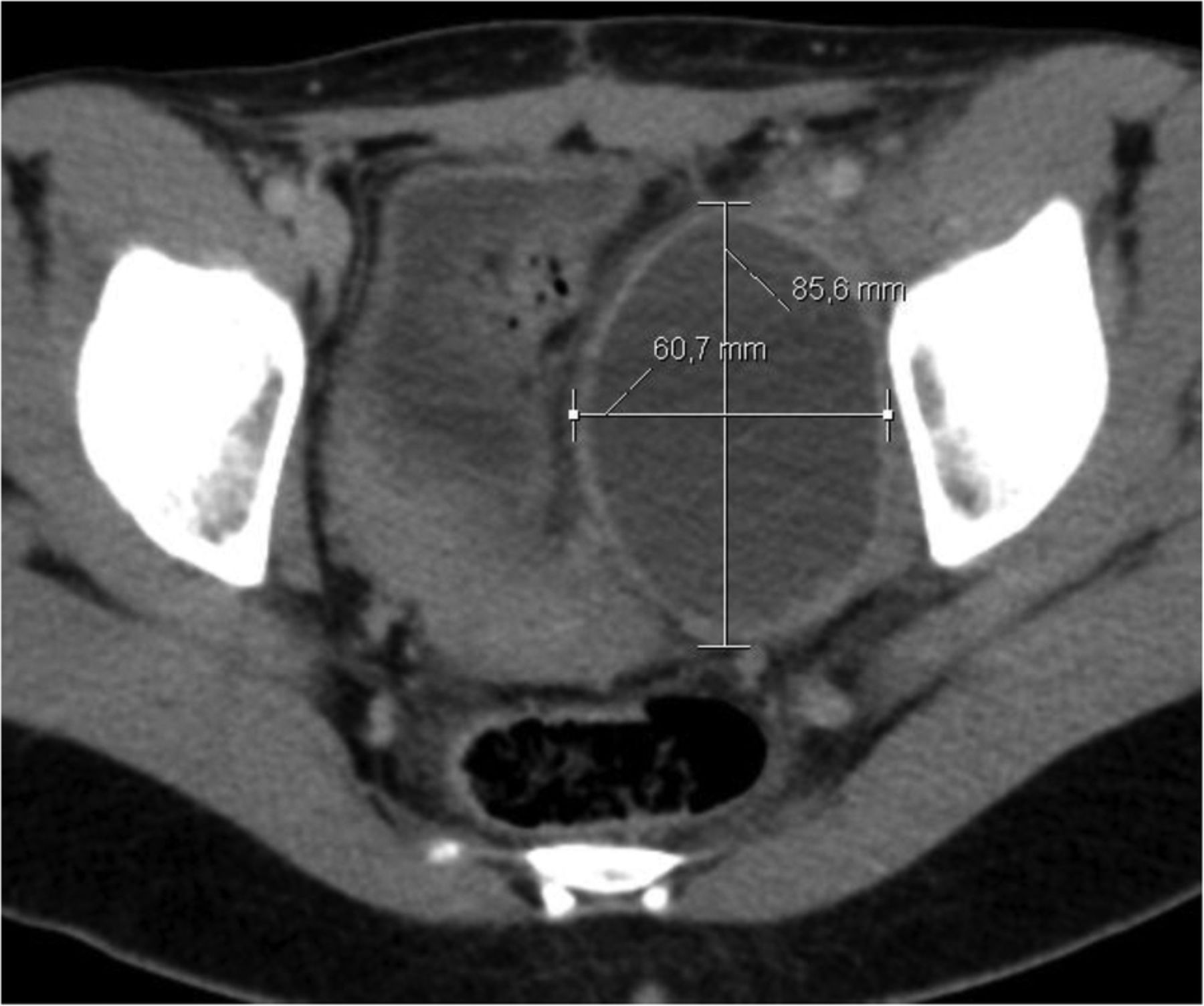
Pelvic CT findings—large cystic left adnexal mass (large anteroposterior diameter of 85.6 mm).
{kind=link}
{kind=link}
{kind=link}
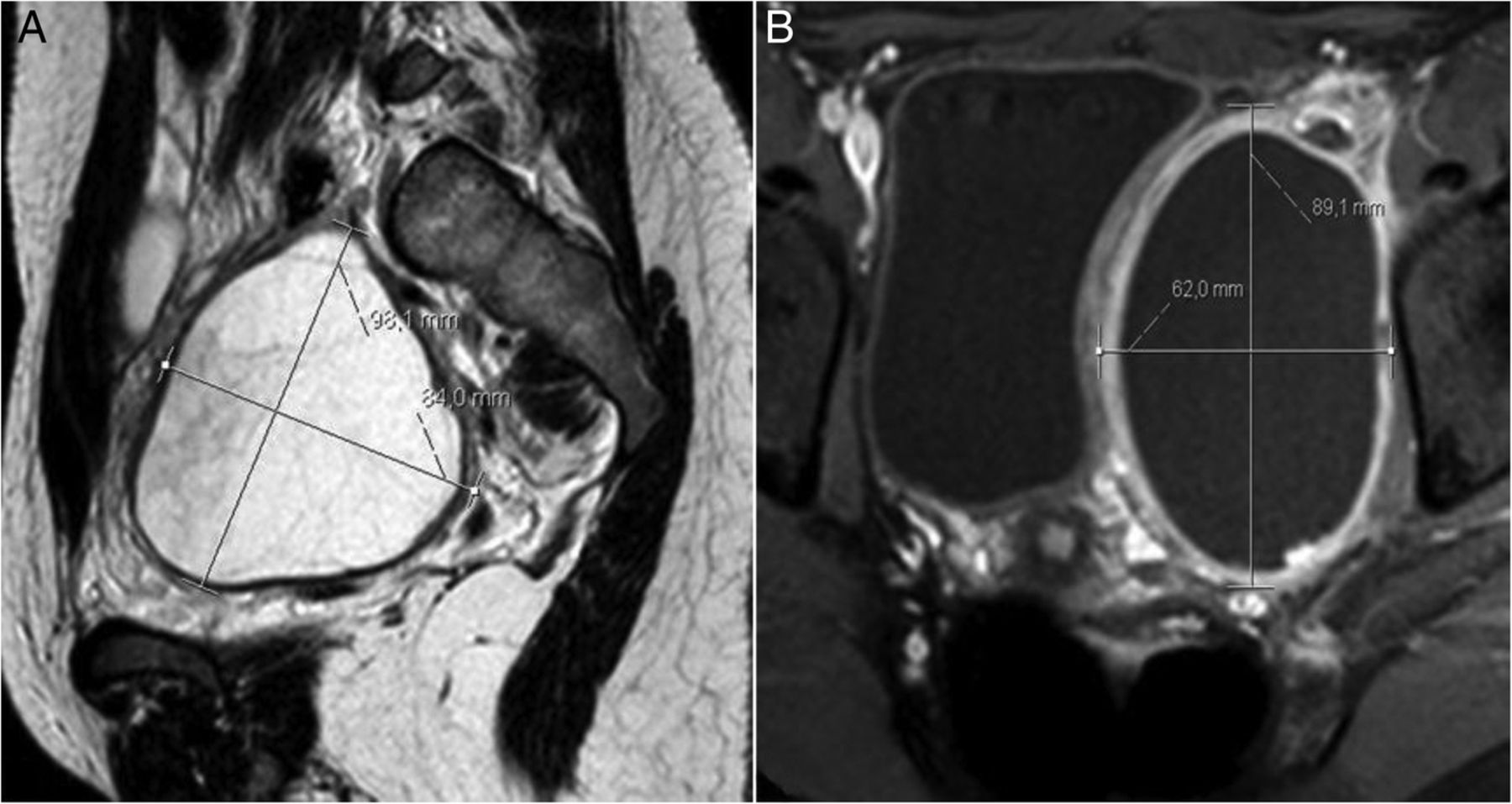
Pelvic MR findings confirming the results of the pelvic ultrasound and CT scan with the differential diagnosis of possible postoperative lymphocoele (A—para-sagittal T2-weighted image showing large cystic left adnexal lesion/lymphocoele containing debris (larger diameter of 98.1 mm); B—axial T1-weighted image showing large cystic thick-walled left adnexal tumour/lymphocoele causing a mass effect on the bladder (large anteroposterior diameter of 89.1 mm)).
The follow-up period for 5 years did not reveal any clinical, analytical (the tumour markers—β-human chorionic gonadotropin, α-fetoprotein, lactate dehydrogenase—were always negative since the initial diagnosis of dysgerminoma) or imaging abnormalities.
Learning points
Ovarian germ cell tumours often present with pain and/or abdominal mass and are usually unilateral, except dysgerminomas, which in 15% of cases are bilateral. Seventy per cent of cases are diagnosed in FIGO (International Federation of Gynaecology and Obstetrics) stage I. Staging is surgical, according to the FIGO staging scheme, common to epithelial tumours. The pelvic recurrence in this type of tumour can occur in 20% of patients, usually in the first 24 months after therapy.1–3
Unilateral salpingo-oophorectomy is a surgical procedure with minimal tumour resection in this type of tumour and is indicated in young women, with the intention of preserving fertility if the uterus and contralateral ovary do not present with abnormalities.2
The current standard treatment of ovarian cancer consists of primary debulking surgery followed by adjuvant chemotherapy. Pelvic and para-aortic lymphadenectomy forms an integral part of the stage surgery and may be associated with intraoperative and postoperative complications (one of the most common postoperative complication is the development of a lymphocoele). So a postoperative lymphocoele should always be included in the differential diagnostic approach to postsurgical pelvic masses appearing after staging ovarian cancer (vs pelvic tumour recurrence or, as in this specific case, co-existing primary bilateral dysgerminoma, with the need for intraoperative evaluation of the contralateral ovary preserved in the primary surgery being imperative).3 Treatment of asymptomatic lymphocoeles is conservative, with these ending up reabsorbed. In the case of bulky infected lymphocoeles, or those associated with pain and compression of adjacent organs, draining, if possible percutaneously, is recommended.
Acknowledgments
The authors would like to thank the Departments of Obstetrics and Gynaecology, and Radiology (Hospital de Braga), for collaborating.
Footnotes
Contributors EV-F, FR, CM and PS evaluated the patient in inpatient clinic. PS followed the patient in outpatient clinic. PS, CM and EV-F performed the surgery. EV-F collected the data and wrote the manuscript. All the authors were involved in the conception of the work and revised it critically for important intellectual content. The authors approved the final version to be submitted/published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.