Article Text

Statistics from Altmetric.com
Description
A 71-year-old man underwent living non-related renal transplantation 5 months prior to presentation. His family brought him to the emergency room with an altered level of consciousness, high-grade fever, vomiting and lower abdominal pain over a period of 8 days. The cause of end-stage renal disease was unknown and he had been on continuous ambulatory peritoneal dialysis prior to the transplantation. His medical history was significant for hypertension, chronic obstructive pulmonary disease and coronary artery disease. He did not have a history of diabetes mellitus nor did he develop post-transplant diabetes mellitus. Immunosuppressive regimen included mycofenolate mofetil, tacrolimus and prednisone but antibody induction therapy was not employed. He underwent transurethral resection of the prostate 2 months earlier for symptomatic benign prostatic hypertrophy. A surveillance urine culture within 2 weeks of the procedure was negative. He was on prophylactic trimethoprim-sulfamethoxazole and had monthly follow-up appointments in the post-transplant clinic where screening urine cultures are performed every visit. There were no documented episodes of urinary tract infection since transplantation. On presentation he was drowsy but arousable and his blood pressure was 86/60 mm Hg with high-grade fever and tachypnoea. CT scan of the abdomen revealed the transplanted kidney appearing significantly enlarged in size with a dilated pelvicalyceal system and ureter with no evidence of obstruction. Strikingly, air was noted within the renal pelvis and ureter. Air was also present within the wall of the renal pelvis, urinary bladder and the seminal vesicles (as seen in figures 1⇓–3). There was no evidence of abscess formation or collection in the abdomen and pelvis. These factors were overall suggestive of emphysematous pyelonephritis (EPN) and cystitis. The CT scan findings for EPN were classified as Class II.1 The patient was evaluated for possible radical allograft nephrectomy, but was deemed inoperable in view of his overall status. He had severe sepsis despite prompt initiation of broad-spectrum antibiotic and escalating inotropic support. Further investigations revealed multiorgan failure and disseminated intravascular coagulation (DIC), eventually leading to death within 24 h of presentation. Owing to severe thrombocytopaenia and DIC, percutaneous catheter drainage was not offered. Blood and urine cultures grew Escherichia coli with extended spectrum β lactamase activity. There is conflicting evidence in the literature as to whether transurethral resection of the prostate (TURP) should be performed before or after transplantation.2 If performed pretransplantation while the patient is oliguric or anuric, bladder neck contracture and/or urethral scarring is a possible complication.3 In other reports—if TURP is performed post-transplantation there is a high risk of urosepsis given the risk of infection with immunosuppression.2 Some authors support performing TURP 6–8 weeks pretransplantation3 ,4 while others advocate that TURP can be performed safely post-transplant when a normal urinary output has been restored.5 When performed post-transplantation, a reduction in immunosuppression for a short period in addition to prophylactic antibiotics is advisable. This case illustrates late presentation of severe emphysematous pyelonephritis and cystitis in a renal transplant recipient with severe sepsis leading to an unfavourable clinical outcome.

CT abdomen and pelvis, coronal plane illustrating enlarged renal allograft with dilated pelvicalyceal system. Air is noted in the pelvis, ureter and bladder wall.

CT abdomen and pelvis, transverse plane highlighting the air noted in the allograft pelvis and ureter.

{kind=link}
{kind=link}
{kind=link}
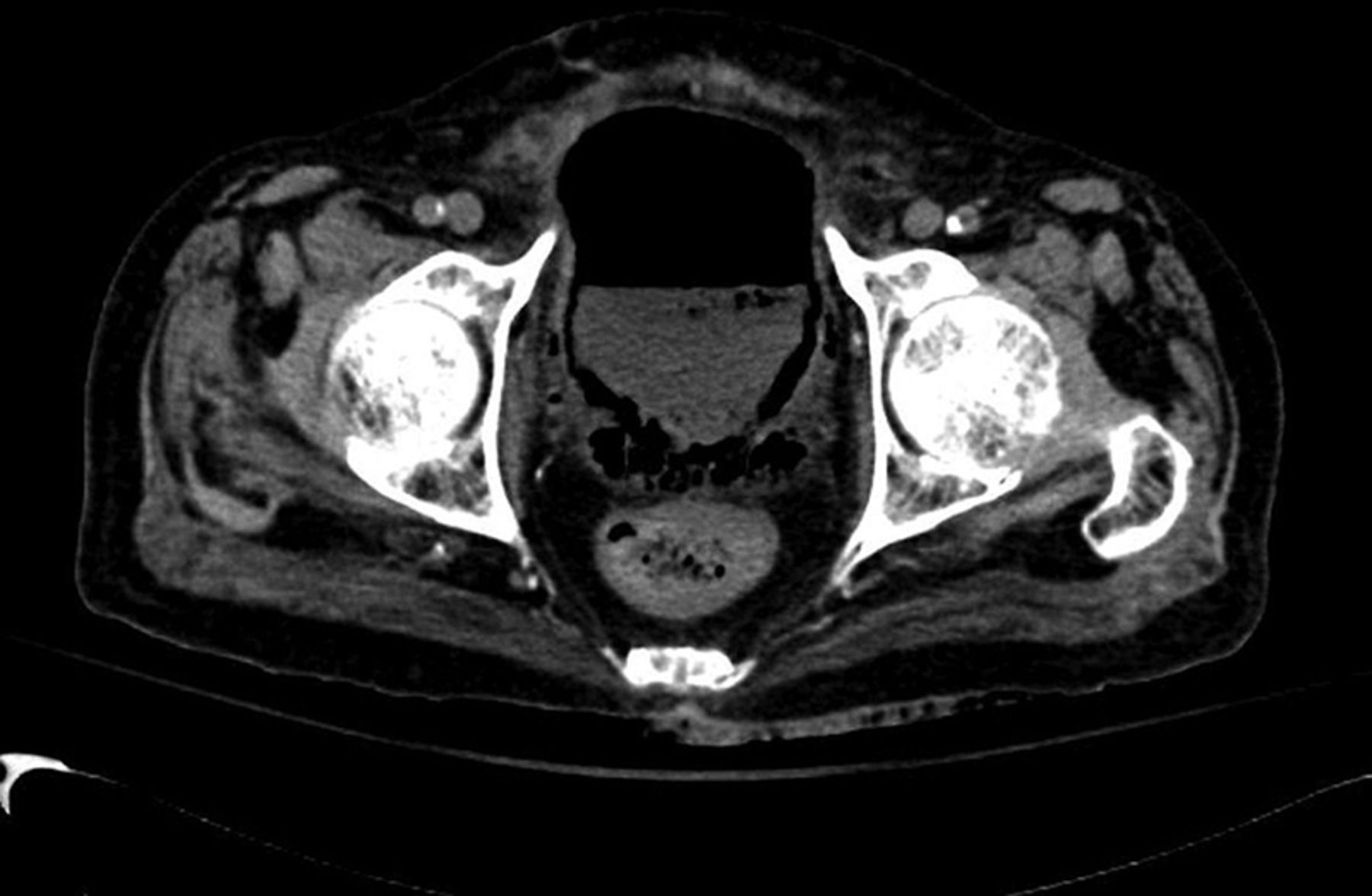
CT abdomen and pelvis, transverse plane illuminating the air present within as well as in the wall of the bladder and in the seminal vesicles.
Learning points
-
Urinary tract infections are common in renal transplant recipients. Risk factors include advanced age, female gender, reflux kidney disease prior to transplantation, diabetes mellitus, cadaveric donor kidney, kidney–pancreas transplant, retransplantation, antibody induction for immunosuppression, urinary bladder catheterisation, history of allograft rejection with subsequent escalation of immunosuppressive therapy and use of ureteral stents.6 ,7
-
Emphysematous pyelonephritis (EPN) is defined as a severe, life-threatening necrotising renal parenchymal infection caused by gas-forming organisms. Escherichia coli (69%) and Klebsiella penumoniae (29%) are the most common organisms that cause EPN, however, other organisms including fungal pathogens have been reported as causative agents.1
-
For patients with Class II1 CT scan findings for EPN, as in our patient, the suggested approach is treatment with broad-spectrum antibiotics plus percutaneous catheter drainage and relief of urinary tract obstruction if present.8
-
Radical allograft nephrectomy is the suggested option in a patient with EPN if the patient's condition is not stabilised within 24–48 h of presentation or if the patient presents with septic shock.9 This procedure should be performed only after consideration of the overall condition of the patient.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.