Article Text

Summary
We present a rare case of an endometrioma present within and firmly adherent to the broad ligament in a patient who experienced an episode of acute abdominal pain. The endometrioma was excised laparoscopically and the broad ligament repaired.
Statistics from Altmetric.com
Background
Endometriosis is a benign condition affecting 6–10% of women of reproductive age, 50–60% of women and teenage girls with pelvic pain, and up to 50% of women with infertility.1 ,2 Endometriomas (cysts lined with ectopic endometrium which are located within the ovary) are found in 17–44% of patients affected by endometriosis.2–4 In this report we present a rare case of an endometrioma present within the broad ligament.
Case presentation
A 32-year-old nulliparous woman presented with a history of severe acute abdominal pain 6 months earlier. At the time of this acute episode 6 months previously, a pelvic ultrasound was undertaken which reported the presence of a cyst (with a high index of suspicion of an endometrioma) separated from the right ovary (which may or may not have been the cause of the acute pelvic pain). The patient stayed in hospital for 2 nights and analgesia was prescribed; no further action was taken.
At current presentation, although she had no ongoing symptoms, the patient sought to have the cyst investigated and removed if appropriate. Examination was unremarkable, and repeat transvaginal ultrasound reported the presence of a right adnexal mass of dimensions 35 mm×23 mm×35 mm within the broad ligament with a well defined smooth border and a wall thickness of 3.5 mm; the centre of the mass had a ground glass appearance.
Treatment
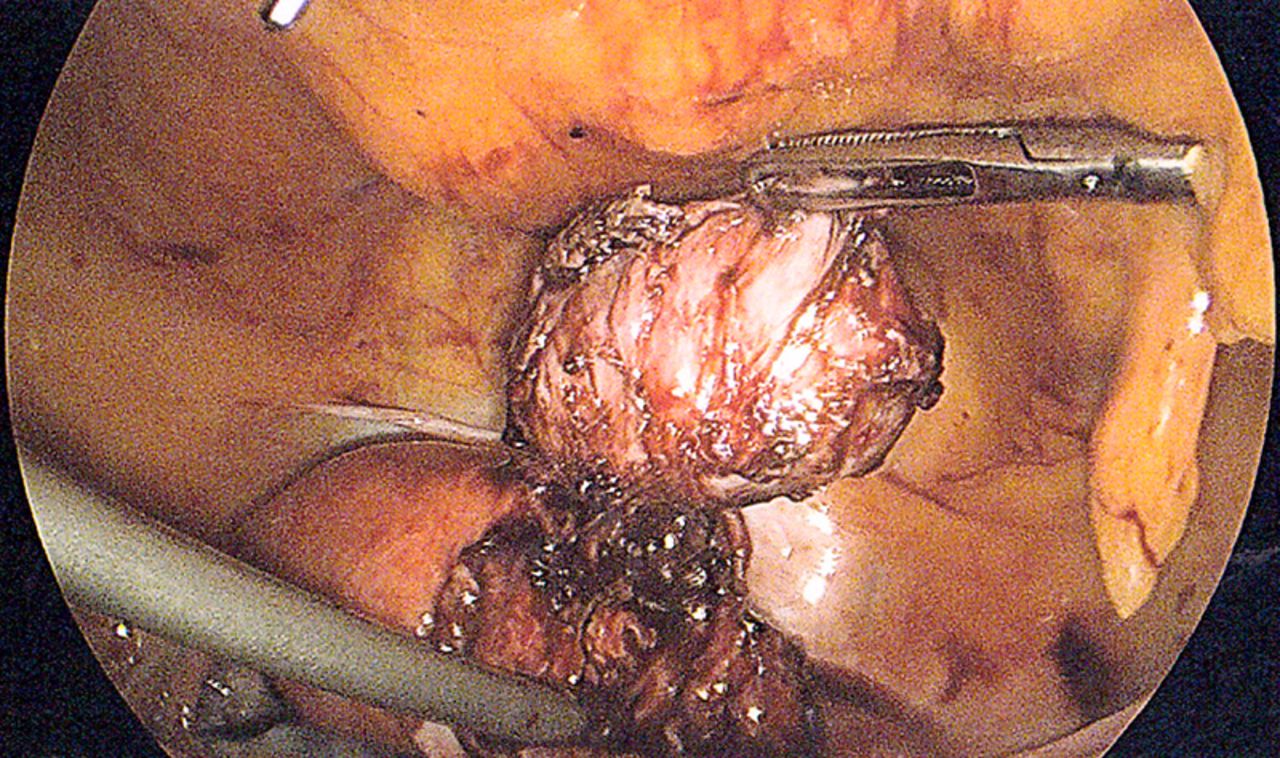
A three-port laparoscopic approach was utilised. The laparoscopic view before dissection is shown in figure 1, which clearly demonstrates the presence of a mass within the broad ligament. This view was perhaps initially suggestive of a subserous uterine fibroid, and hence it was at this point thought that perhaps the ultrasound findings were due to cystic degeneration of a subserous fibroid.

Laparoscopic view showing the presence of a mass within the broad ligament.
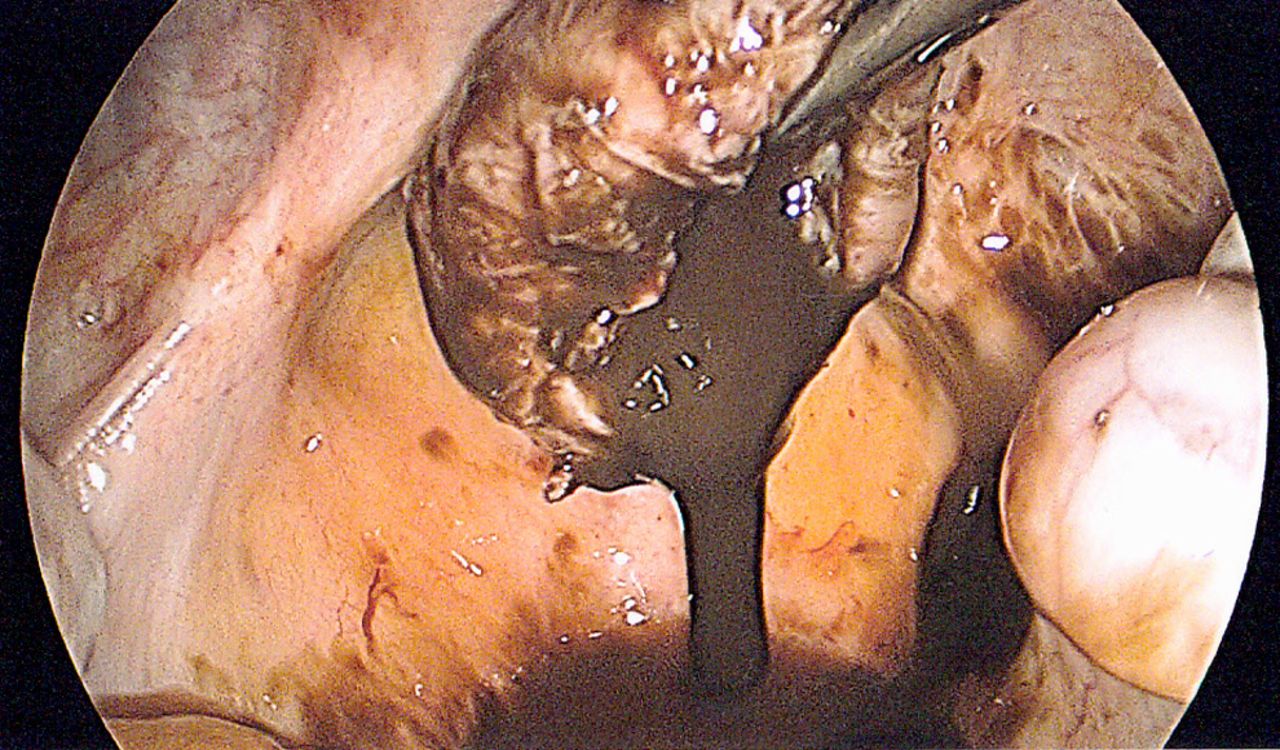
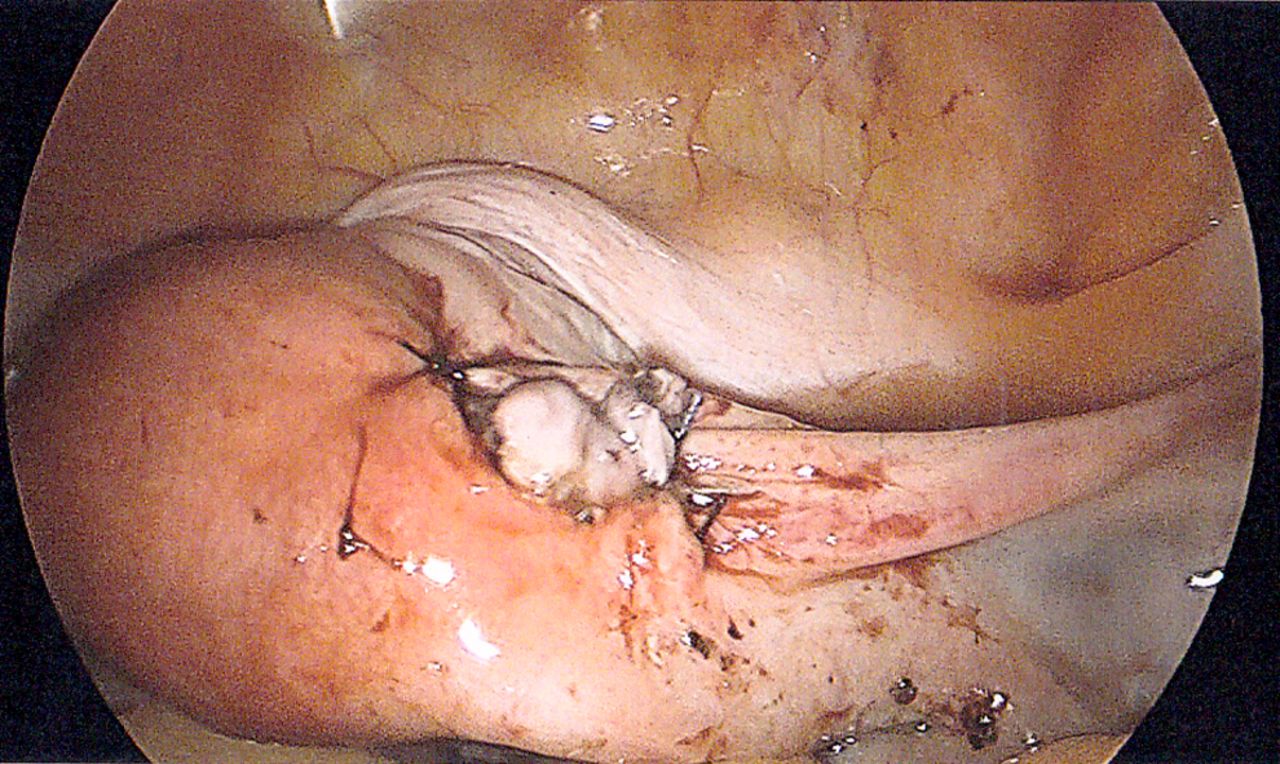
Upon dissection it was apparent that the mass was indeed a thick-walled cyst which was within and firmly adherent to the broad ligament. The cyst was fully excised (figure 2). The cyst was then opened in order to drain the ‘chocolate’ material contained within the cyst into the pouch of Douglas so as to allow removal of the cyst wall from the pelvic cavity via the 5 mm laparoscopic port (figure 3). The ‘chocolate’ material was aspirated and the pelvic cavity thoroughly irrigated with saline. The broad ligament was repaired with three interrupted sutures (figure 4).
Excision of the cyst.
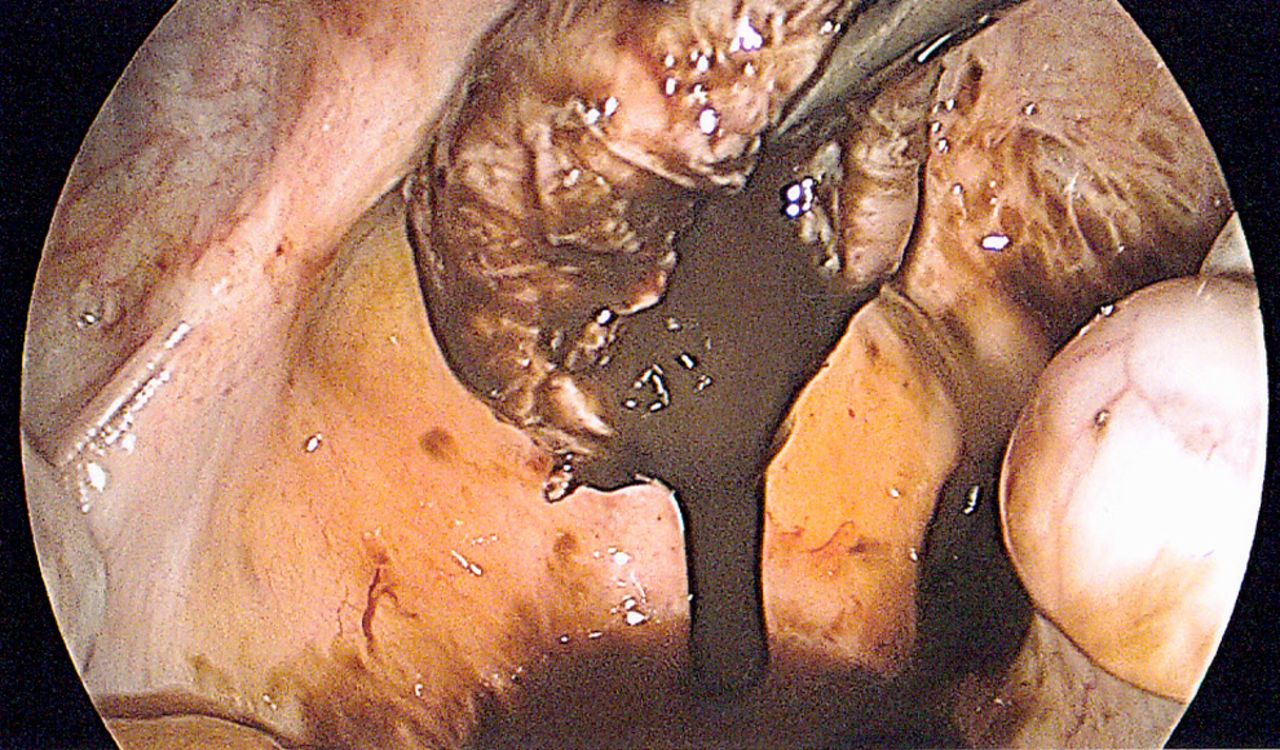
Drainage of the ‘chocolate’ fluid from the cyst.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The defect in the broad ligament has been repaired with three interrupted sutures.
Both ovaries were unremarkable in appearance. No other endometriosis was present within the pelvic cavity, although a small nodule on the left uterosacral ligament was identified; a biopsy of this section of tissue revealed the presence of chronic inflammation (but no endometriosis) on histological examination.
Histological examination of the cyst wall found fibrous tissue lined in part by haemosiderin-laden macrophages and cells with an appearance of endometrial stroma, confirming the diagnosis of an endometrioma. A biopsy was also taken from the nodule in the left uterosacral ligament.
Outcome and follow-up
No surgical complications were experienced and the patient was discharged after an overnight hospital stay.
Discussion
Only three cases of an endometrioma specifically within the broad ligament have been reported,5 ,6 although there has also been one previous case of a solid and cystic mass of endometriosis within the broad ligament,7 and another of adenomyosis within the broad ligament.8
The rare possibility of endometriosis in cyst form or otherwise should be borne in mind during imaging and laparoscopy. Complete excision of the endometrioma leaving no residual tissue (as opposed to just drainage for instance) should be undertaken, as the situation is likely to be similar to ovarian endometriomas where drainage only without excision is associated with a high incidence of recurrence.9 ,10
The location of this endometrioma is also of note regarding the aetiology of endometriosis. The most prominent theory for the origin of endometriosis is that of retrograde menstruation which states that during menstruation, some endometrial cells reflux into the pelvic cavity and within the peritoneum.11 It has been suggested that ovarian endometriomas may be the result of retrograde menstruation followed by invagination of surface endometrial cells.12 ,13 With great insight, Whitehouse, in his description of a similar mass almost a century ago, noted that the fact that the endometrioma was present between the layers of the broad ligament with no communication with the peritoneal cavity suggests that it must have arisen by a mechanism other than retrograde menstruation6 (which we can now speculate may be from Müllerian remnants14 or coelomic metaplasia15). A variety of evidence suggests that endometriosis can arise through mechanisms other than retrograde menstruation,16 and indeed retrograde endometriosis is unlikely to account for the endometrioma described in this case.
Learning points
-
Endometriomas can rarely be present within the broad ligament.
-
Management is via laparoscopic excision and broad ligament repair.
-
The location of this endometrioma deep within the broad ligament provides further evidence supporting the suggestion that the aetiology of endometriomas can (at least in some cases) be explained by methods other than retrograde menstruation.
References
Footnotes
-
Correction notice This article has been corrected since it was published online: 21 May 2014. The authors names have been corrected.
-
Contributors AT undertook the literature search and prepared the manuscript. AKT saw the patient in clinic and performed the operation described.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction