Article Text

Statistics from Altmetric.com
Description
A 42-year-old man presented with productive cough, haemoptysis, night sweating, temperature 39°C, asthenia and weight loss of 35 kg in 12 months. He had a 25-year history of smoking (40 cigarettes/day) and alcoholism. Laboratory tests showed normochromic normocytic anaemia (haemoglobin 8.8 g/dL, red blood cell 2.72×106/mmc, and mean corpuscular volume 100), neutrophilic leucocytosis and white cell count 17 78×103/mmc). Chest CT scan revealed an excavated lesion in the apico-dorsal segment of the left upper lobe (65×70 mm) with solid vegetation inside, delimitated by a thick wall with polylobate edges, and the suggestive presence of ‘halo sign’ (figure 1). The solid vegetation was characteristically movable changing the body position (figure 2). Video bronchoscopy showed the presence of purulent secretions from the left upper lobe bronchus with easily bleeding mucosae. Results of microbiological examination were normal. Although the bronchial biopsy showed metaplastic and thickened plate epithelium, focal parakeratosis, mild dysplasia and leucocyte exocytosis, the diagnosis of pulmonary aspergilloma (PA) was highly suspected. The patient underwent left upper pulmonary lobectomy with mediastinal lymphadenectomy. The final histology confirmed the presence of a large aspergilloma (figure 3A–C). The patient was discharged on the sixth postoperative day. The patient is asymptomatic at 16 months of follow-up.
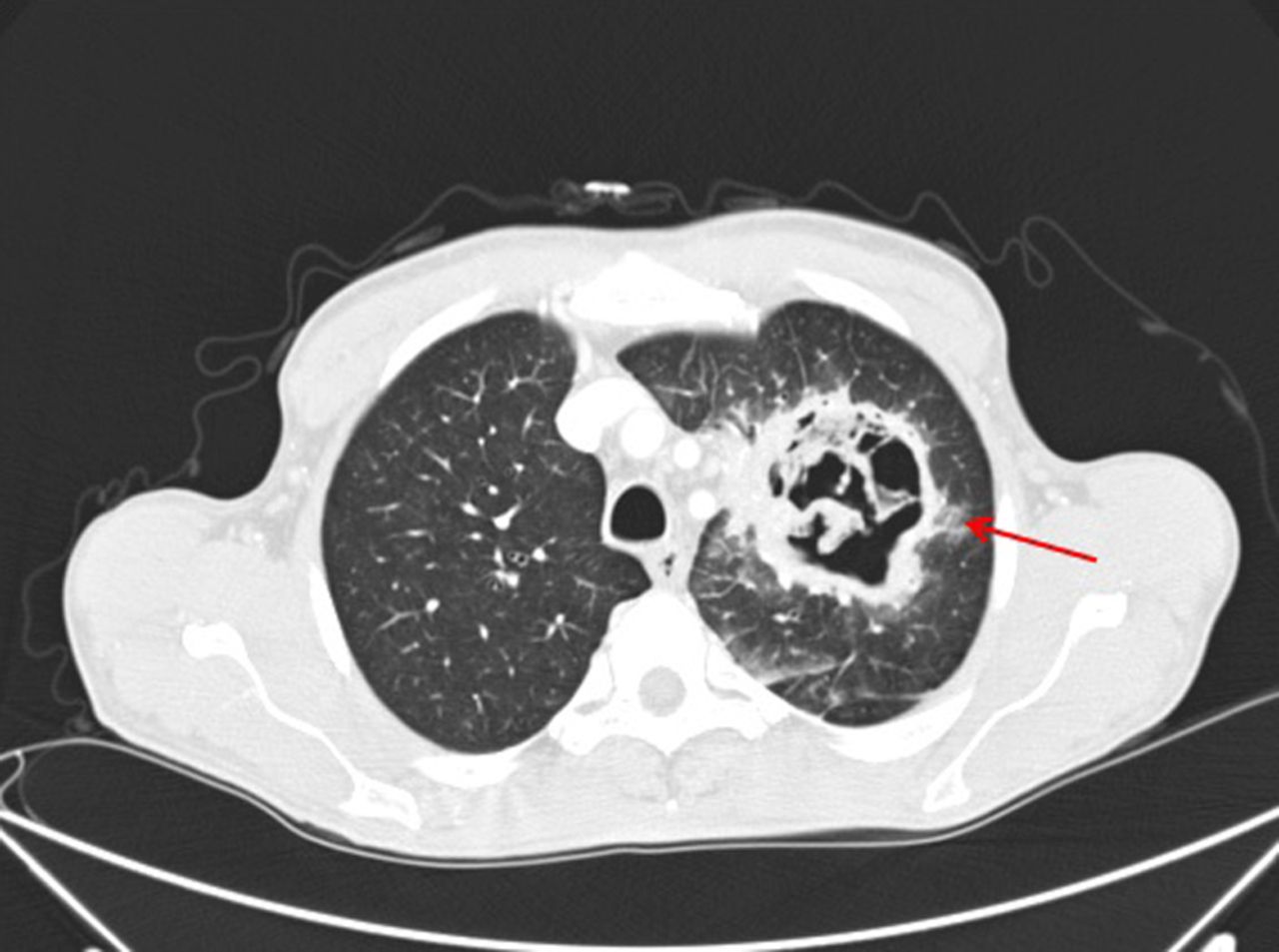
Axial chest CT. A large excavated lesion in the apico-dorsal segment of left upper lobe (65×70 mm) bounded by thick wall with poly-lobed margins; the arrow indicates the ‘halo’ sign.
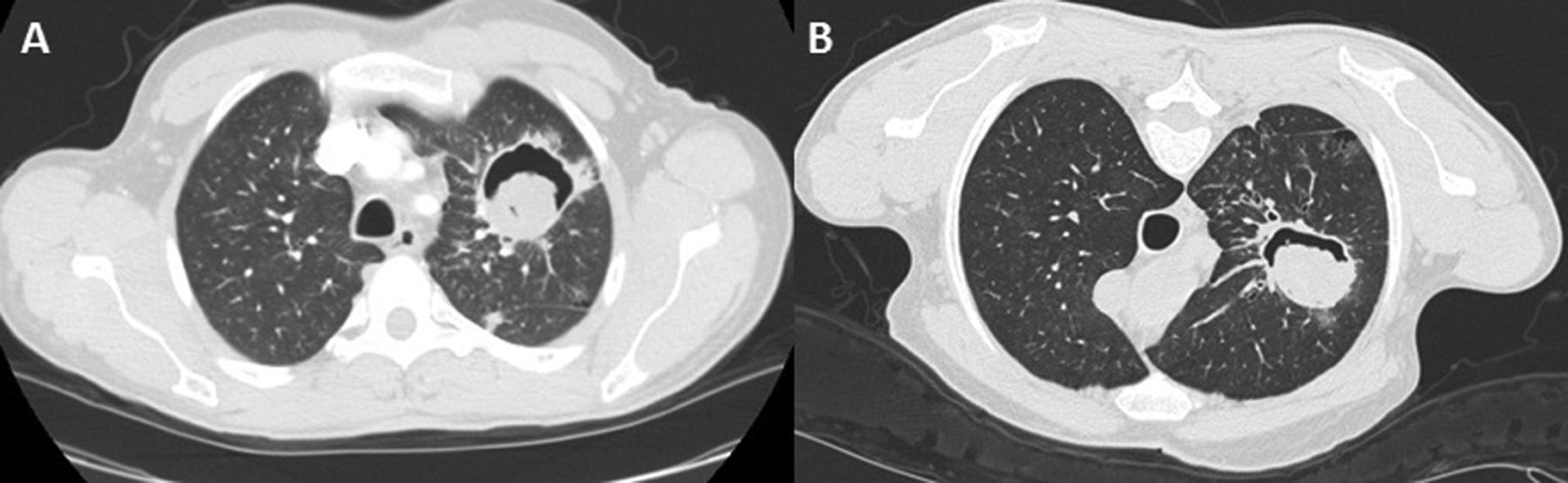
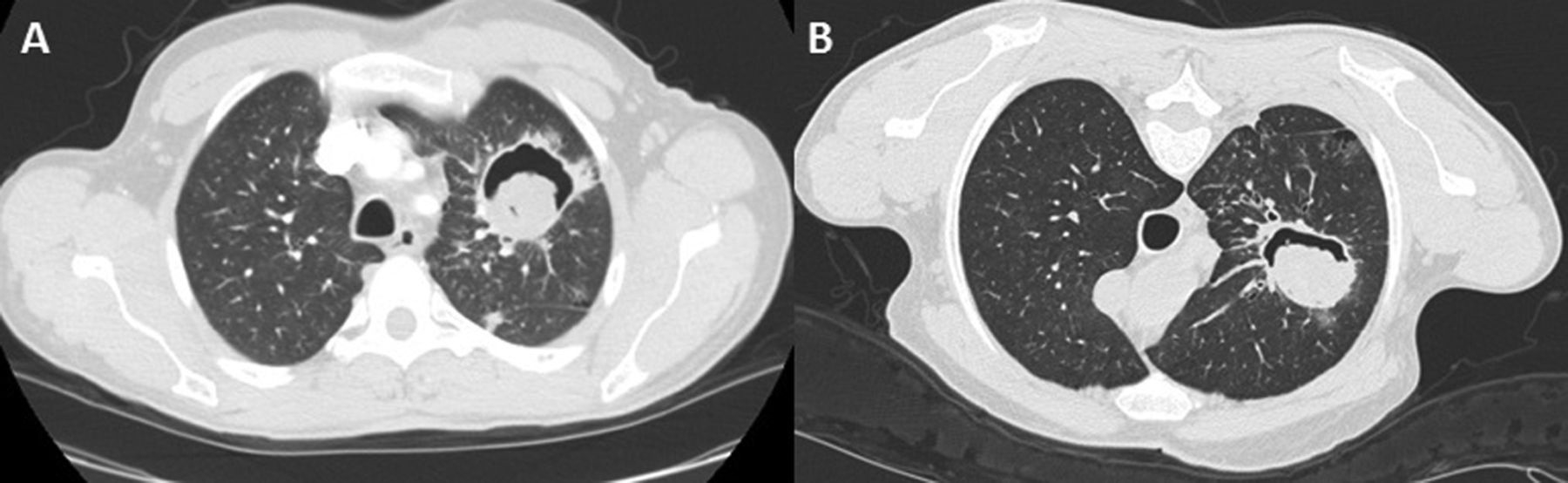
Axial chest CT in supine (A) and prone (B) position. The solid vegetation is movable changing the body position.

{kind=link}
{kind=link}
{kind=link}
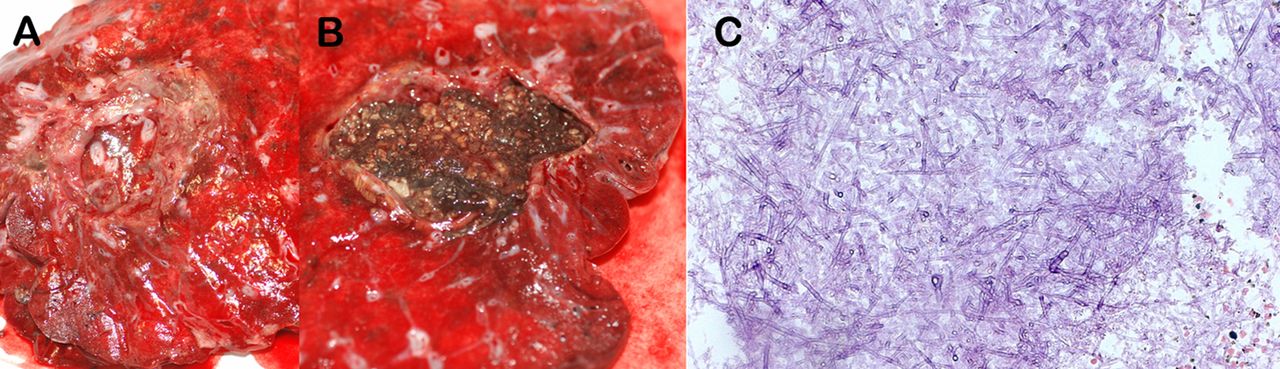
(A and B) Macroscopic specimen; and (C) histopathological examination with H&E. (A) Perilesional fibrosis; (B) the presence of cavities with necrotic-purulent content; and (C) fungal hyphae and spore.
The diagnosis of PA is challenging, and a multidisciplinary approach as for other diseases is encouraged.1 Although the bronchoscopy was unable to identify the causative agent in our patient, generally it plays a central role not only for the diagnosis of PA but also for therapeutic interventions.2
A classic radiographic appearance of PA is a cavity containing a solid, round and often mobile intracavitary fungus ball. Another CT characteristic is the presence of the halo sign which refers to a zone of ground-glass attenuation surrounding a pulmonary nodule or mass on CT images, and may be the first evidence of pulmonary fungal infection.3 ,4 In conclusion, the contemporary presence of both these CT findings make the diagnosis of PA especially truthful.
Learning points
-
Although not always evident, the presence of a mobile vegetation inside a lung cavity is highly suggestive of pulmonary aspergilloma.
-
CT halo sign is also highly suggestive of pulmonary fungal infection.
-
The contemporary presence of both these CT findings makes the diagnosis of pulmonary aspergilloma very accurate.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.