Article Text

Statistics from Altmetric.com
Description
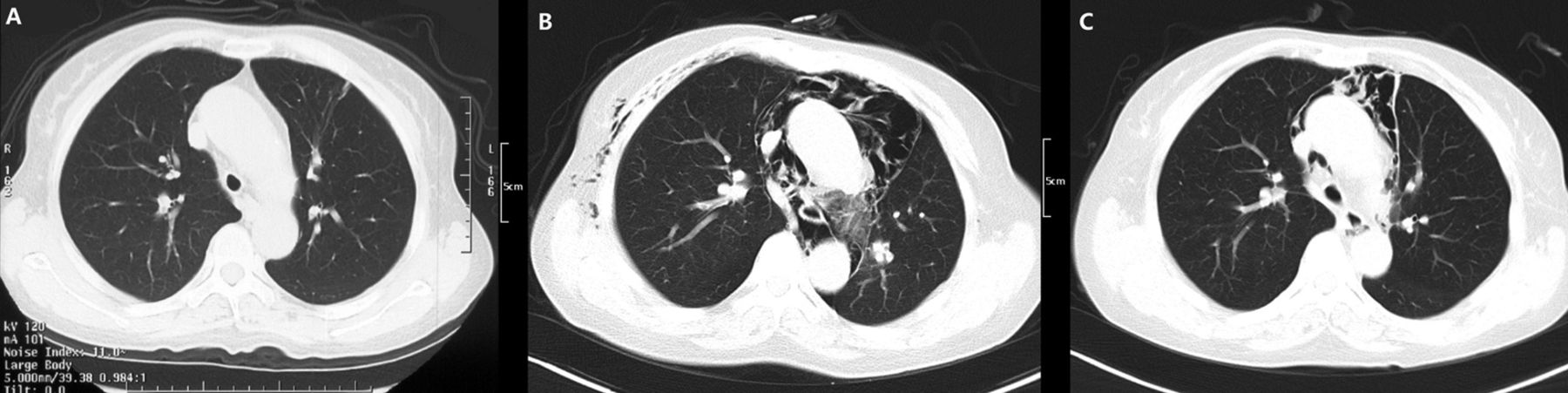
A 50-year-old woman presented to our department with a 6-year history of recurrent dyspnoea and cough. Six year ago she started to have external ear and nasal pain, episcleritis and dyspnoea. She was diagnosed with relapsing polychondritis (RP). Her disease was under control after treatment with a high dose of oral prednisone (1 mg/kg/day) and intravenous cyclophosphamide. The patient experienced a flare of respiratory symptoms 3 months before admission and her prednisone dose was increased to 60 mg/kg/day. A CT scan of the chest showed only airway stenosis of trachea and bilateral main bronchi, but with mostly clear lung fields (figure 1A). However 3 weeks before admission the patient presented with severe dyspnoea, cough and stridor again, the dose of the prednisone was then tapered to 50 mg/kg/day. The patient reported no trauma or other medical history. On admission, physical examination revealed sibilant wheezing sound on the entire lung field. Laboratory findings demonstrated increased serum levels of white cell count and erythrocyte sedimentation rate. CT of the chest showed pneumomediastinum, bilateral pneumohypoderma and slight left-sided pneumothorax (figure 1B). The patient was treated with a high dose of intravenous methylprednisolone therapy and cyclophosphamide. Her symptoms relieved quickly and a repeated CT scan preformed after 1 week showed significant improvement of the pneumomediastinum and pneumohypoderma (figure 1C).
{kind=link}
(A) Trachea stenosis, tracheal wall thickening and almost clear lung fields. (B) Pneumomediastinum, bilateral pneumohypoderma and slightly left-sided pneumothorax were shown in CT of the chest. (C) Result of the repeated CT scan showing significant improvement of the pneumomediastinum and pneumohypoderma after 1 week of treatment.
RP is an immune-mediated and multisystem disease that causes progressive inflammatory destruction of the cartilage.1 About one-third of the RP cases have airway involvement, including constriction and malacia in the trachea and relatively large bronchi, which is usually associated with a worse prognosis.2 However, pneumomediastinum has been rarely reported in RP except in patients who underwent intervention for airway problems or had underlying pulmonary fibrosis or bullae.3 If the symptoms of pneumomediastinum develop in a patient with RP as in our case, the diagnoses of the relapse of RP or pulmonary infections would be more easily suspected. It was supposed that the rupture of the damaged tracheal cartilage might contribute to the air leak in our case.
Learning points
-
Dyspnoea, cough and stridor are the most common respiratory symptoms of relapsing polychondritis, which is usually associated with constrictions of the trachea or main bronchi.
-
Pneumomediastinum is an uncommon pulmonary presentation of relapsing polychondritis and it should be considered when patients with RP are presented with dyspnoea.
Footnotes
-
Contributors YJ and SW collected the clinical information, treated the patient and wrote the manuscript.
-
Funding This study was funded by Beijing Nova Program (2008B49).
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.