Article Text

Statistics from Altmetric.com
Description
A 47-year-old man was admitted to a hospital after developing acute severe right hip pain upon standing up from a kneeling position. He was unable to bear weight and had no history of recent trauma. X-rays showed suspected right neck of femur fracture in an abnormal femur.
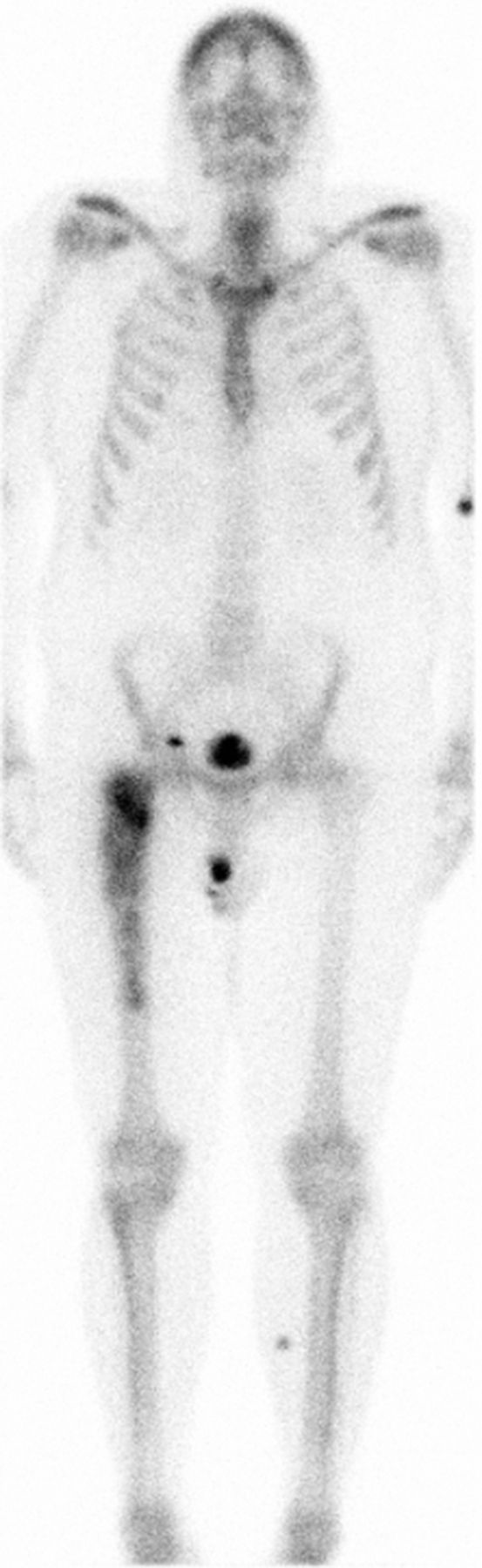
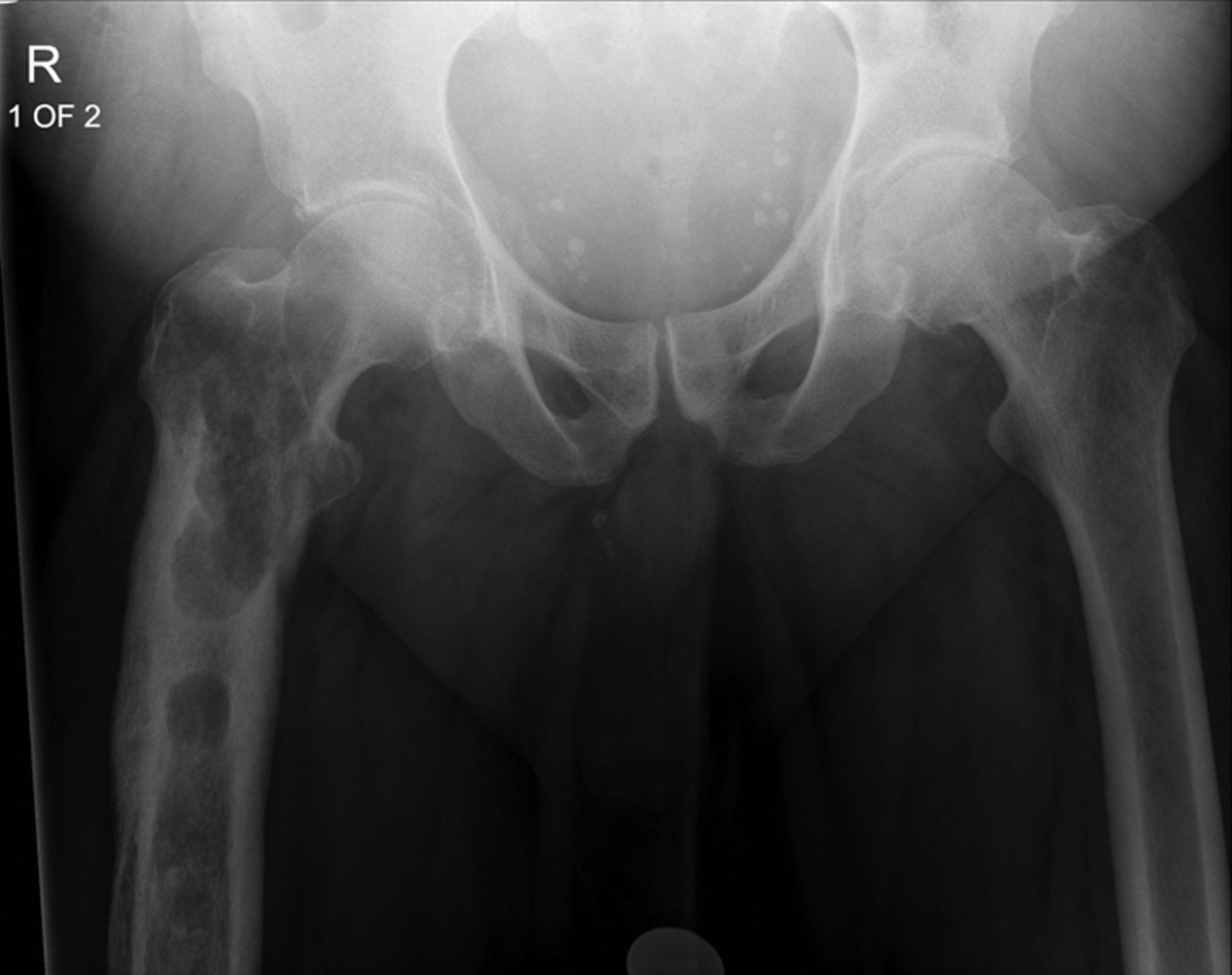
He was noted to have a history of 6 months of right thigh pains, causing occasional antalgic gait. He had been investigated prior to his acute admission with plain X-ray radiographs, MRI and dynamic isotope scan. His X-rays and MRI were suggestive of either chronic osteomyelitis, fibrous dysplasia or a benign tumour (figures 1 and 2). The T2-weighted MRI showed a breach in the cortex of his femur, suggesting a bone infection rather than dysplasia (figure 3).1 His isotope bone scan showed increased uptake localised to his right proximal femur—where his pains were—suggestive of an infection or tumour (figure 4).
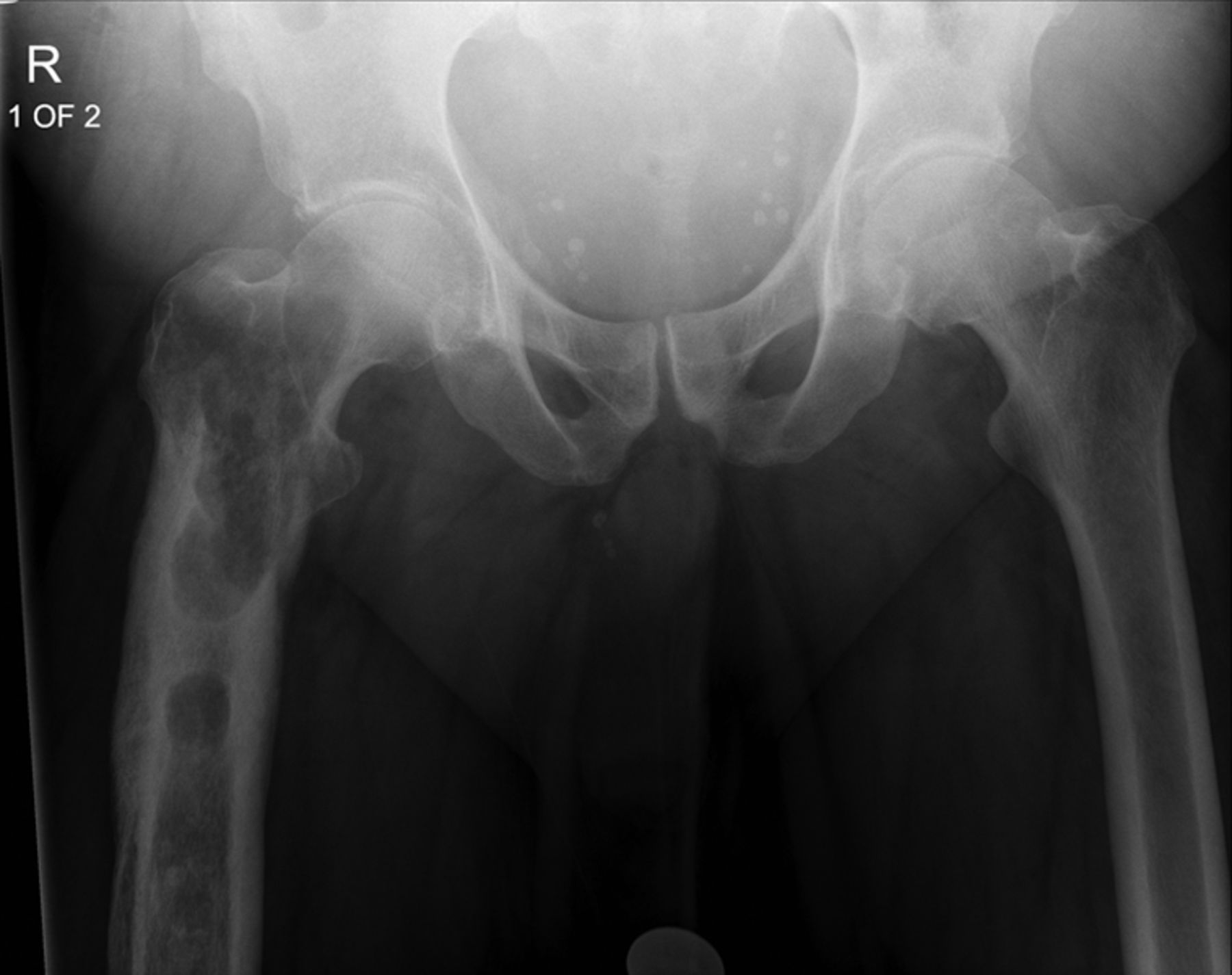
Antero-posterior pelvis X-ray before acute admission showing fibrous dysplasia of the right proximal femur.
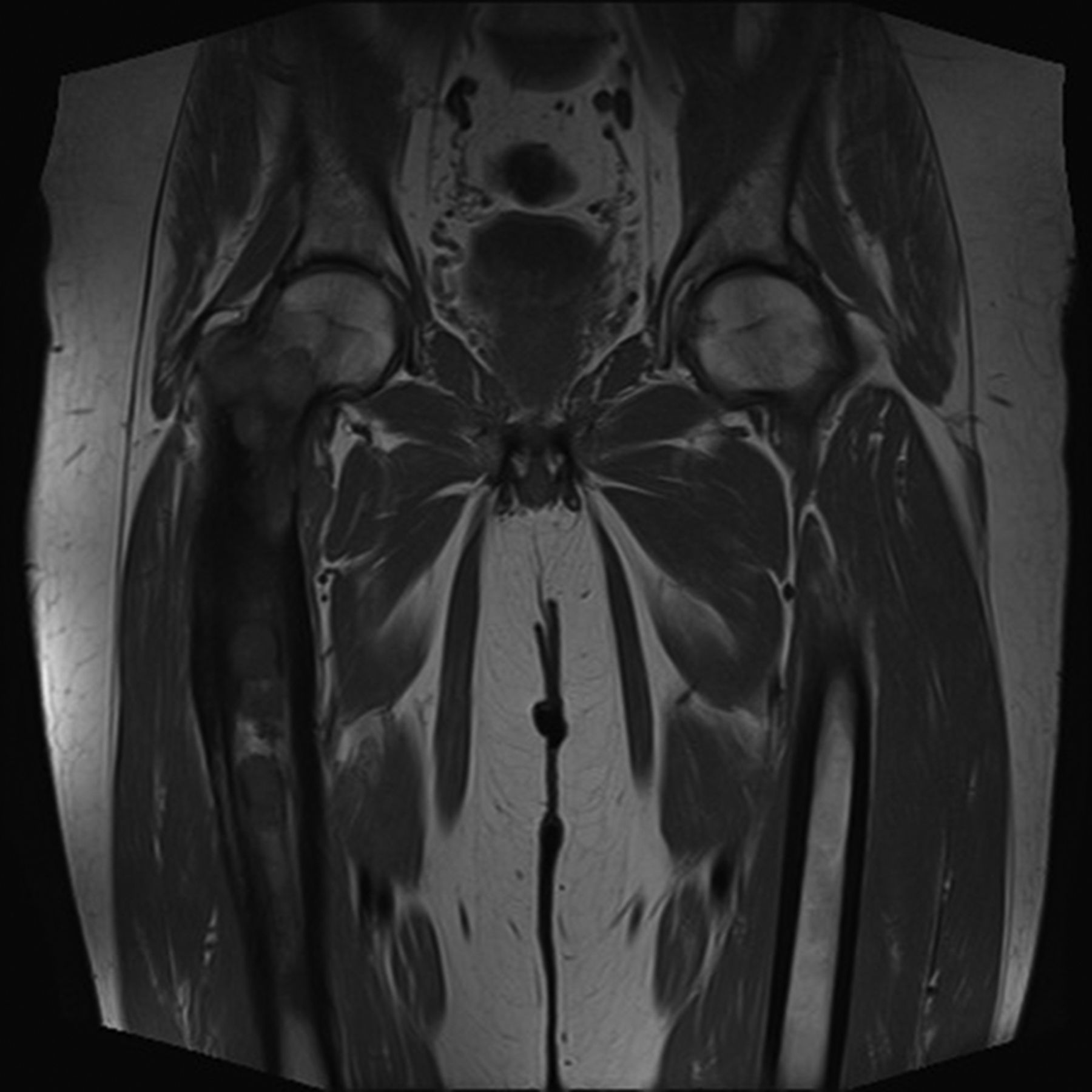
Antero-posterior pelvis MRI before acute admission showing fibrous dysplasia of the right proximal femur.

Axial MRI (T2) of proximal femurs showing suspected fluid breaching cortex of right femur.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Isotope bone scan showing increased uptake (‘hot’ area) in right proximal femur.
He was deemed to have a pathological fracture; however, surgical intervention was delayed until a definitive diagnosis was made. If he did indeed have an infection, then any prosthetic implants or open reduction and internal fixation would be contraindicated. His pain was controlled with traction, and he underwent a right proximal femur biopsy and hip aspiration to confirm his diagnosis. He remained as an inpatient for 10 days for analgesia and traction while awaiting histology and microbiology results.
Ultimately microbiology tests were negative for infection and histological analysis excluded tumour and confirmed a diagnosis of fibrous dysplasia.
He was therefore treated with a long-stem total hip replacement to good effect.
Learning points
-
Fibrous dysplasia should be considered as a differential diagnosis in pathological fractures.
-
Radiological features of fibrous dysplasia may be confused with malignancy or infection.
-
Fibrous dysplasia rarely breaches the cortex of the bone, unless due to a pathological fracture.
-
‘Hot’ areas on dynamic bone scan are suggestive of infection or tumour. Fibrous dysplasia can also be ‘hot’ on bone scan depending on cellularity.
-
Establishing diagnosis is vital before the definitive treatment of a pathological fracture.
Reference
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.