Article Text

Statistics from Altmetric.com
Description
A 28-year-old man was admitted with slurred speech and right arm and leg weakness. His medical history revealed repetitive aphthous oral ulcerations. Brain MRI showed lesions on pons extending to bilateral middle cerebellar peduncles (figure 1). Diffusion-weighted imaging (DWI) showed hypointensity in mid-pons with high apparent diffusion coefficient (ADC) value (1.817×10−3 mm2/s; figure 2A) and hyperintensity in left pons with low ADC value (0.66×10−3 mm2/s) compared with the ADC value of lesion-free pons (0.99×10−3 mm2/s; figure 2B).
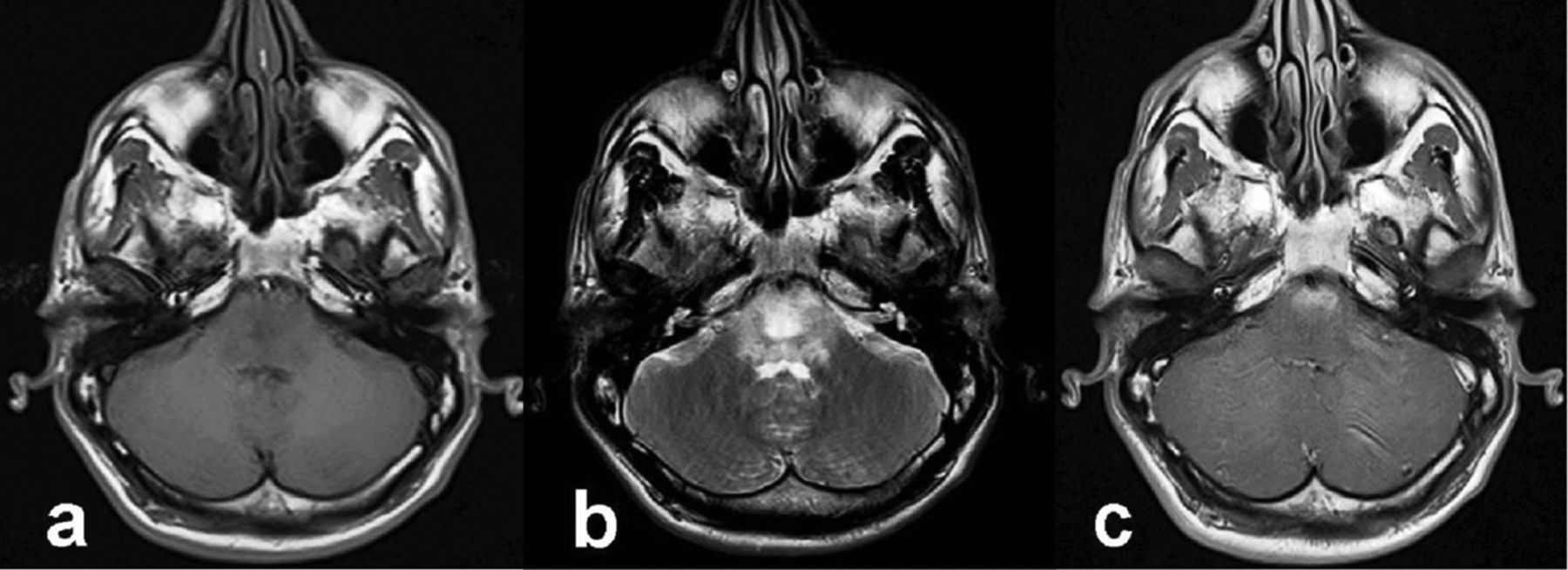
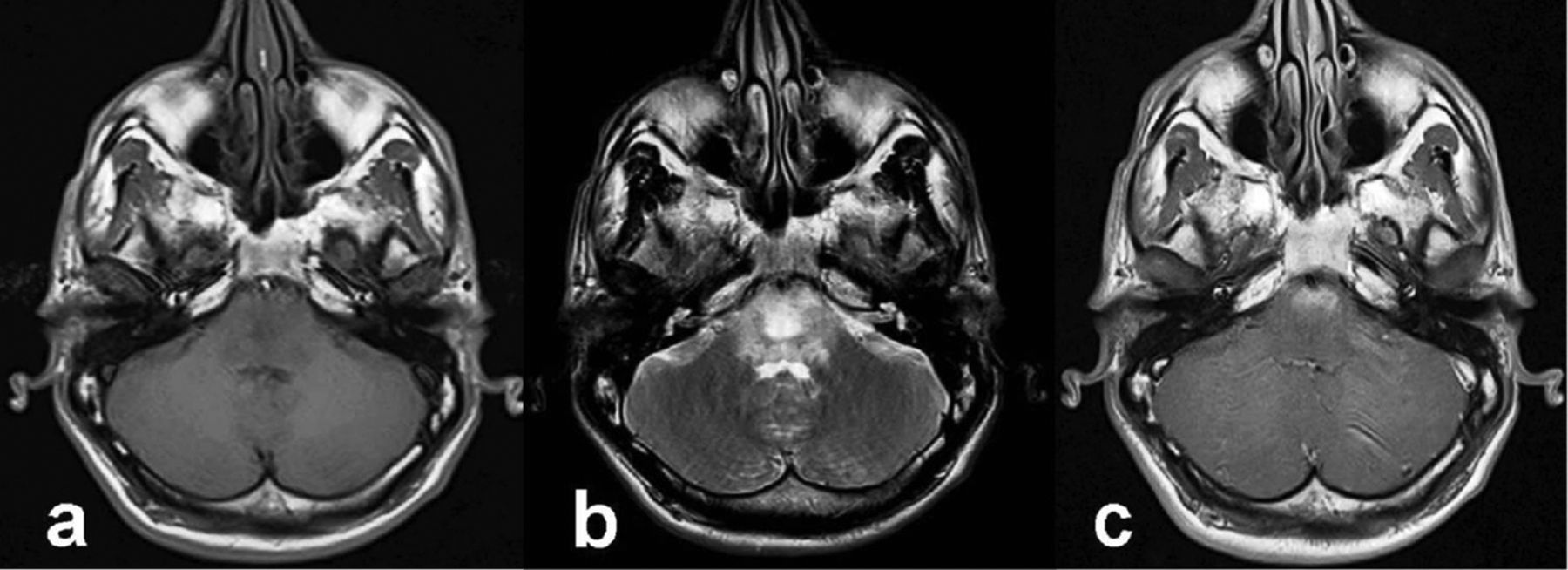
Brain MRI shows lesions in the pons extending to bilateral middle cerebellar peduncles, which are hypointense on T1-weighted imaging (A), hyperintense on T2-weighted imaging (B), with heterogeneous contrast enhancement (C).
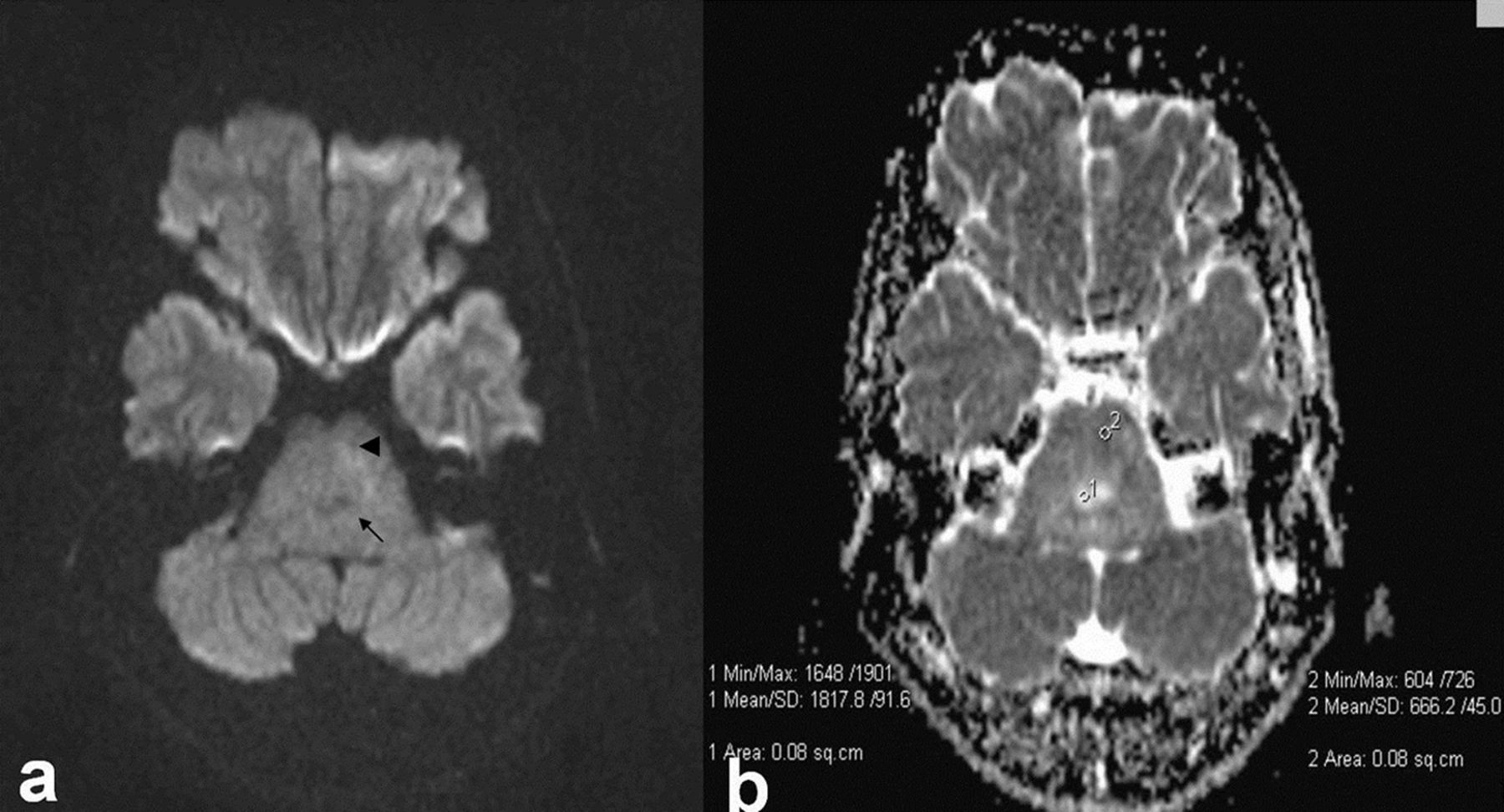
(A) Diffusion-weighted imaging shows low signal intensity in central part of pons (arrow), high signal intensity on left side of the pons (arrowhead). (B) Apparent diffusion coefficient map shows vasogenic oedema in central part of pons (arrow), cytotoxic oedema on left side of the pons (arrowhead).
The patient was diagnosed with Behçet's disease with incipient genital ulcers; brainstem lesions were regarded as acute neuro-Behçet's disease (NBD) lesions. A follow-up MRI at eighth month has shown almost complete resolution of lesions, with small focus in pons and has shown coexistent brainstem and cerebellar atrophy after the steroid therapy. Follow-up DWI showed no abnormality, but a high ADC value (1.22×10−3 mm2/s) was noted in hyperintense lesion on T2-weighted imaging (T2WI) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Follow-up T2-weighted imaging (T2WI) shows (A) high signal intensity in the pons (arrow), (B) brain stem and cerebellar atrophy and (C) apparent diffusion coefficient map shows gliosis/demyelination on the of pons.
NBD can be defined as meningoencephalitis with predilection for brainstem, basal ganglia and thalamus, subcortical white matter damage and spinal cord lesions.1 Well-known conventional MRI features of acute/subacute parenchymal NBD include hyperintense lesions on T2WI with contrast enhancement on T1-weighted imaging. These lesions tend to resolve or decrease in size in the chronic phase.2 The DWI findings in NBD are (A) hyperintensity with ADC values (possibly due to vasogenic oedema and vasculitis) in acute/active disease2 and (B) hyperintensity on DWI with decreased ADC value (due to cytotoxic oedema following ischaemic changes caused by vasculitis) in subacute NBD.3 Furthermore, chronic lesions may show high ADC values consistent with demyelisation or reactive gliosis.2
Learning points
-
Neuro-Behçet's disease (NBD), is one of the most devastating manifestations of the Behçet's disease.
-
Diffusion-weighted imaging (DWI) might help in differential diagnosis of acute brainstem NBD lesions with revealing the vasogenic oedema.
-
It is important to know the possibility of other DWI findings in NBD.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.