Article Text

Statistics from Altmetric.com
Description
Single ventricle (SV) defects, including common inflow of both the atria emptying into one ventricle, occur at an incidence of 0.05–0.1/10 000 live-births.1 Common atrium is a rare variety of interatrial communication which forms a type of endocardial cushion defect characterised by deficient atrial septum, the vestigial remnants sometimes remain as diaphanous strands of tissue.2 ,3 Common atrium is very rarely seen in patients with SV.3 In patients with common atrium and SV, there is mixing of arterial and venous blood in the common cardiac chamber which causes severe cyanosis and hypoxia in these patients.3 ,4
We report the case of a 6-month-old female baby who presented with central cyanosis, dyspnoea along with difficulty in feeding, fatigue and irritability since the neonatal period. She was the result of a full-term, caesarean delivery with an uneventful antenatal and perinatal course with no other obvious external malformations. She was the first-born child and her parents had no history of prior conception. The baby had a body weight of 6 kg and an oxygen saturation of 73% at room air. The auscultatory findings included a single first and second heart sound and soft grade II/VI ejection systolic murmur on physical examination. An initial working diagnosis of a complex cyanotic congenital heart disease with an admixture physiology was considered.
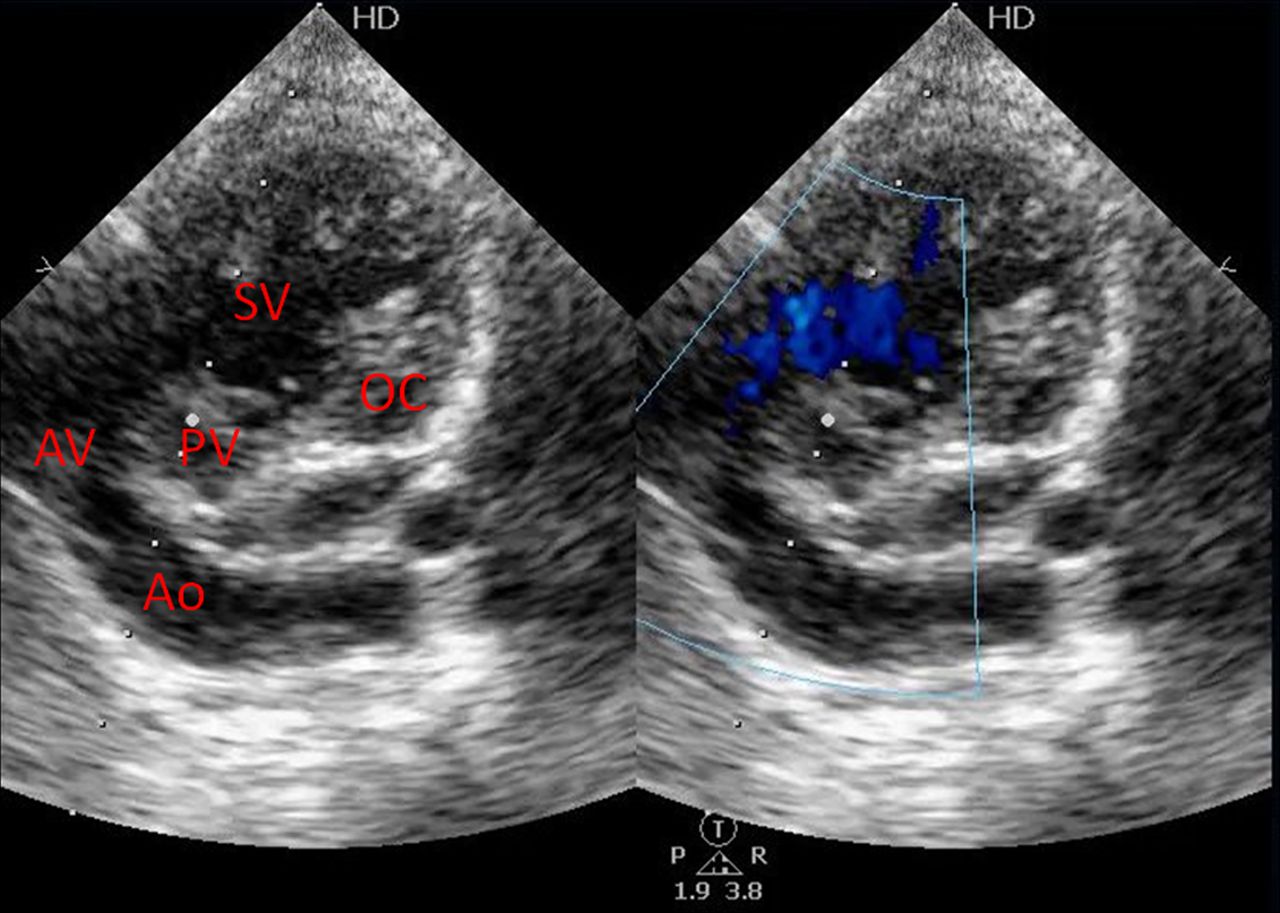
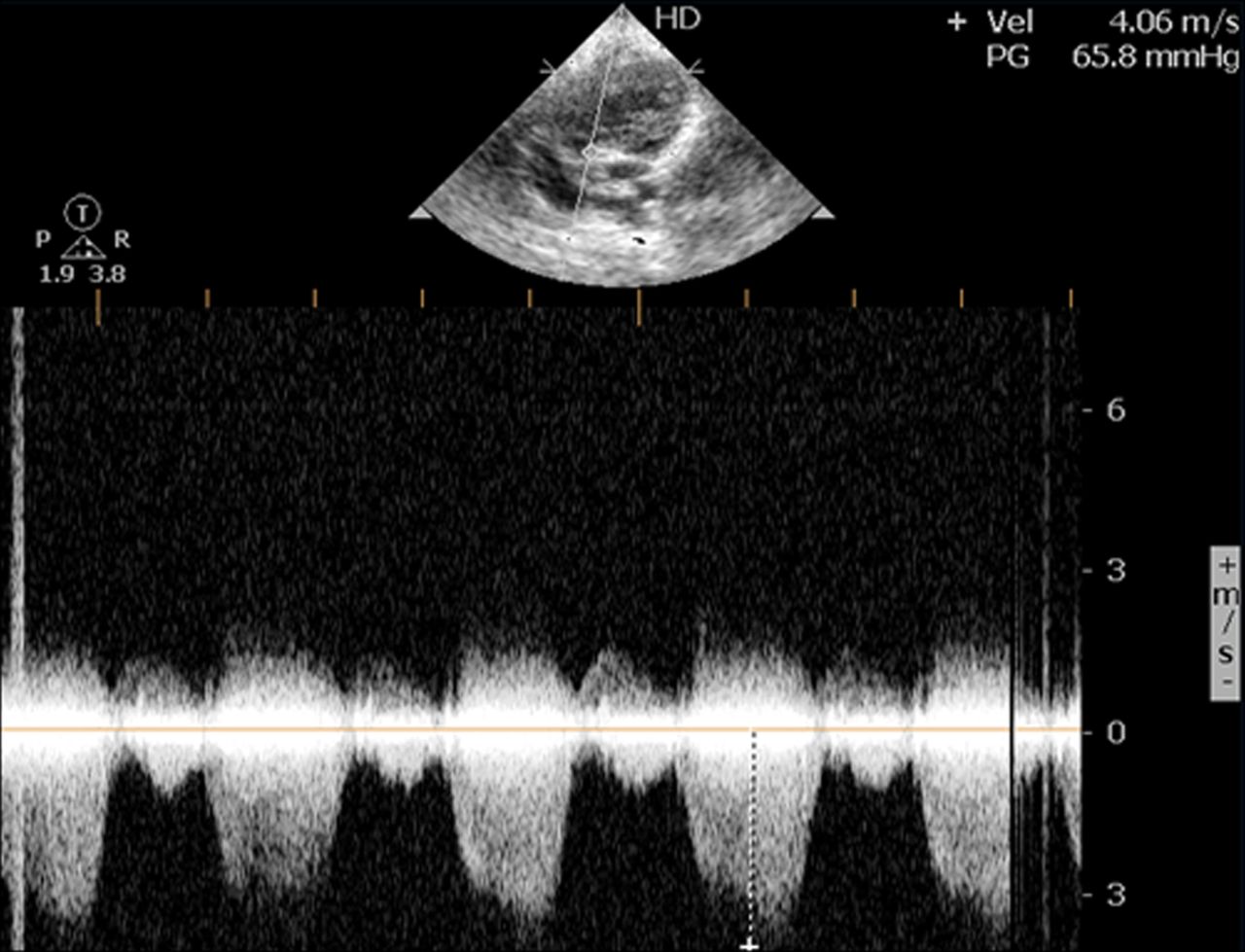
Echocardiogram revealed a common atrium and SV of left ventricular morphology with inverted outlet chamber (OC) (figure 1; video 1). There was concordant relation of the major arteries with the aorta arising from morphological left ventricle (LV) and hypoplastic pulmonary artery arising from OC (figure 2; video 2). The patient had an infundibular stenosis with gradient of 65 mm Hg (figures 3 and 4).

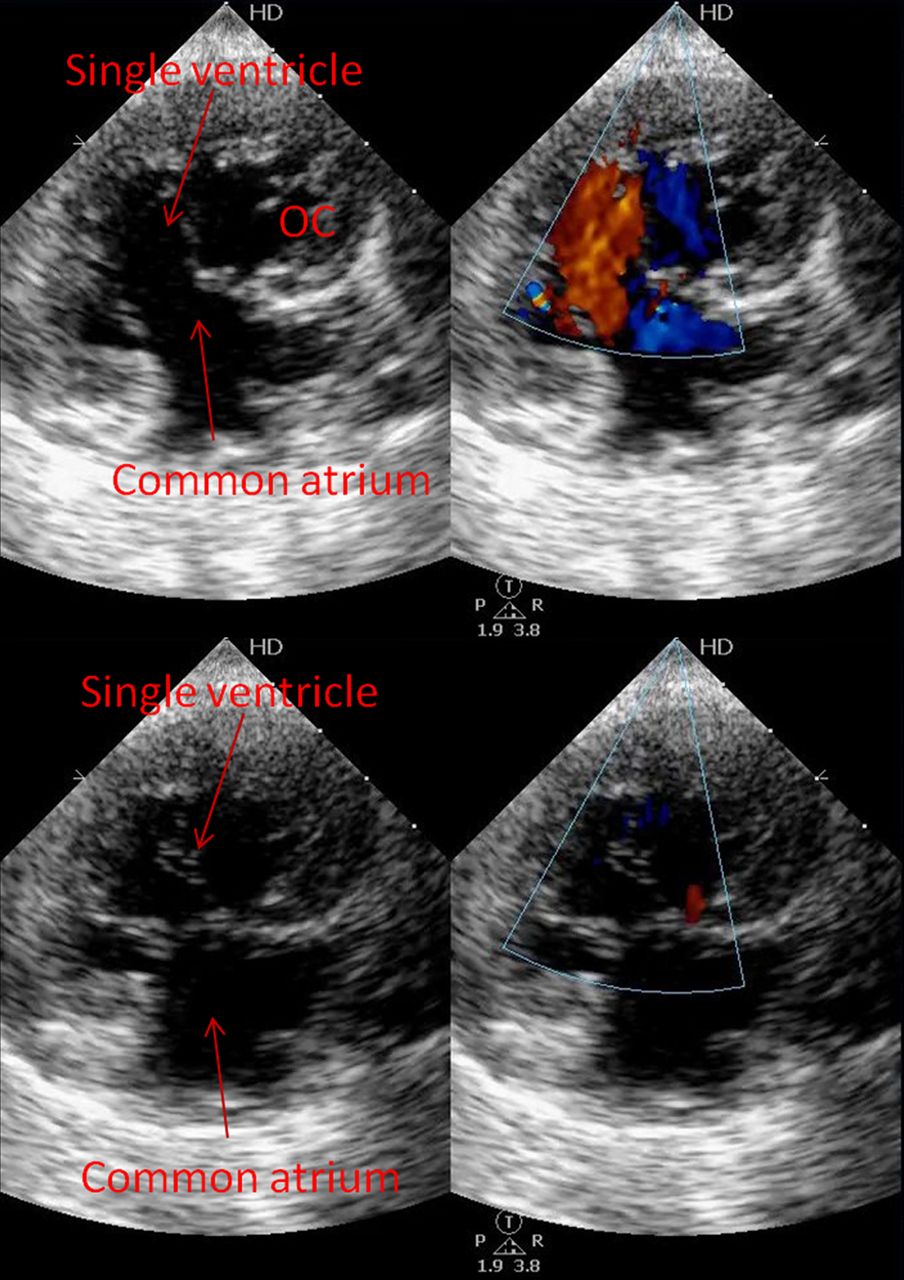
Apical 4-chamber view with colour compare image in diastole and systole shows common atrium, single ventricle and inverted outlet chamber.
Apical 4C view with colour compare shows common atrium, single ventricle and inverted outlet chamber.
Modified 4-chamber view shows aorta arising from morphological left ventricle and hypoplastic pulmonary artery arising from outlet chamber.
Modified 4C view shows aorta (Ao) arising from morphological left ventricle and hypoplastic pulmonary artery arising from outlet chamber.

Continuous wave Doppler at pulmonary valve shows infundibular stenosis with gradient of 65 mm Hg.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
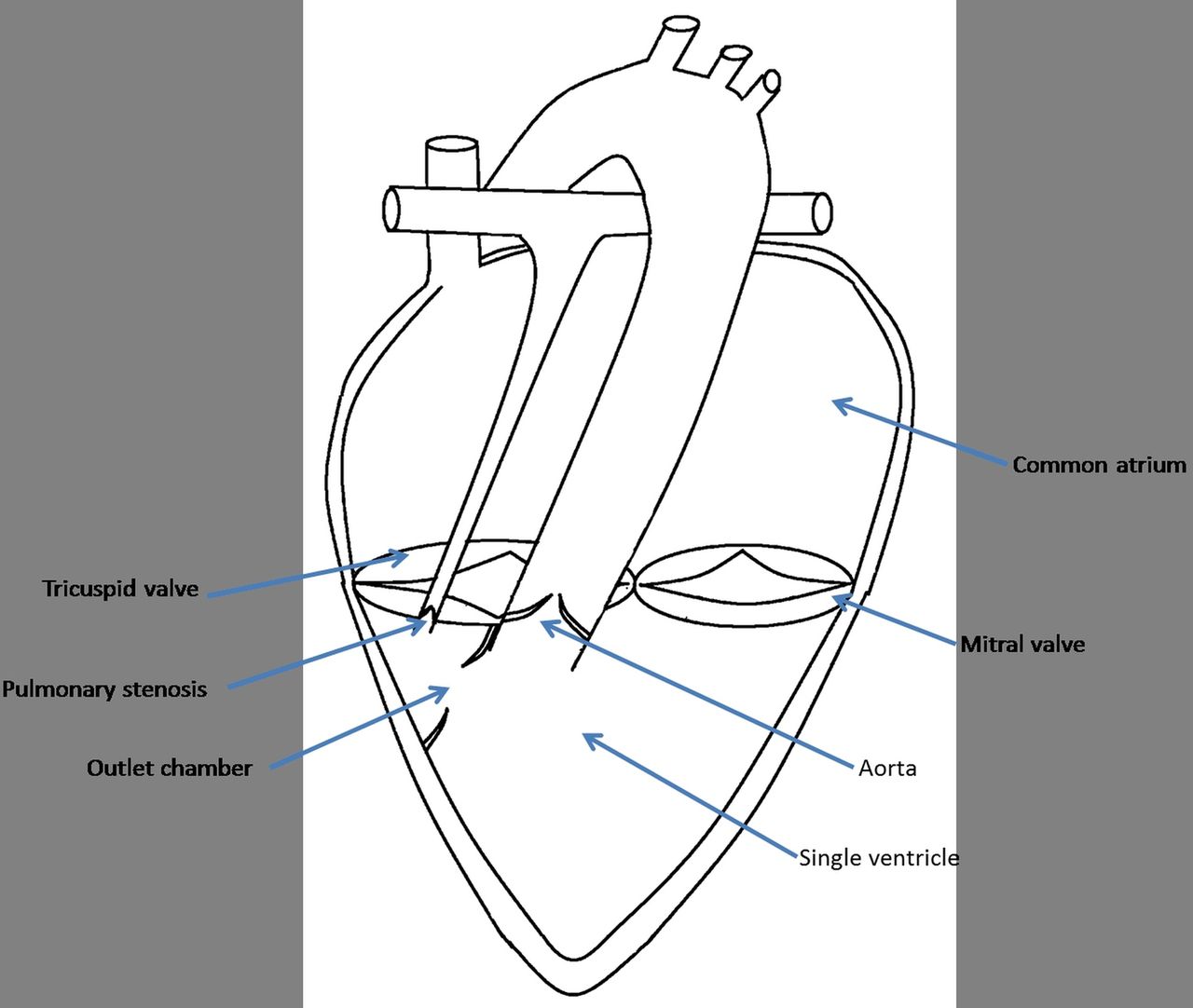
Illustrated line diagram of the patient's heart indicating the common atrium and single ventricle.
The patient underwent a palliative Blalock-Taussig shunt (BT shunt) surgery and was stable at 3 months of follow-up and was planned for a palliative Glenn shunt at the age of around 10–12 months and subsequently a Fontan surgery at an age of around 3–4 years. Presently, the infant is maintaining saturation of around 85% and the gain of weight is appropriate for her age and has minimal symptoms, which are acceptable for a complex cyanotic congenital heart disease having undergone a palliative repair.
This case mimics a single-chambered heart in a human being. The prognosis of SV with common atrium is poor with high mortality rate of up to 50% in infancy. The median survival of single ventricle of LV morphology is 14 years, while that of the right ventricle morphology is 4 years. Patients having decreased pulmonary blood flow situation usually need a modified Blalock-Taussig shunt while those with increased blood flow may require a pulmonary artery banding procedure. This is usually followed up by a bidirectional Glenn operation as the second-stage after 3–6 months and a subsequent Fontan procedure at 2–3 years. Cases having complicated ventricular and arterial morphology and obstructed bulboventricular foramen may require complex surgical therapy, which is usually individualised according to the requirement of the case. The Fontan surgery is usually considered the definitive treatment for such cases which provides significantly improved prognosis as compared with the natural history of the disease. The surgical mortality of each case depends on the complexity of the lesion and the type of surgery planned at each stage of presentation and may range from 5% to 10% at each stage.
Learning points
-
Single ventricle defects are rare and can present in various morphological forms which include cases with increased or decreased blood flow, and the association of another rare entity in the form of common atrium makes this case exceptional.
-
Prompt surgical correction with initial palliation along the Fontan pathway, as was performed for this case, can ultimately lead to relatively better long-term outcome and survival compared with the natural history of the disease.
-
High index of suspicion and echocardiography early in infancy is the key to appropriate management and can be lifesaving in such cases with complex cyanotic congenital heart disease as in this case.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.