Article Text

Statistics from Altmetric.com
Description
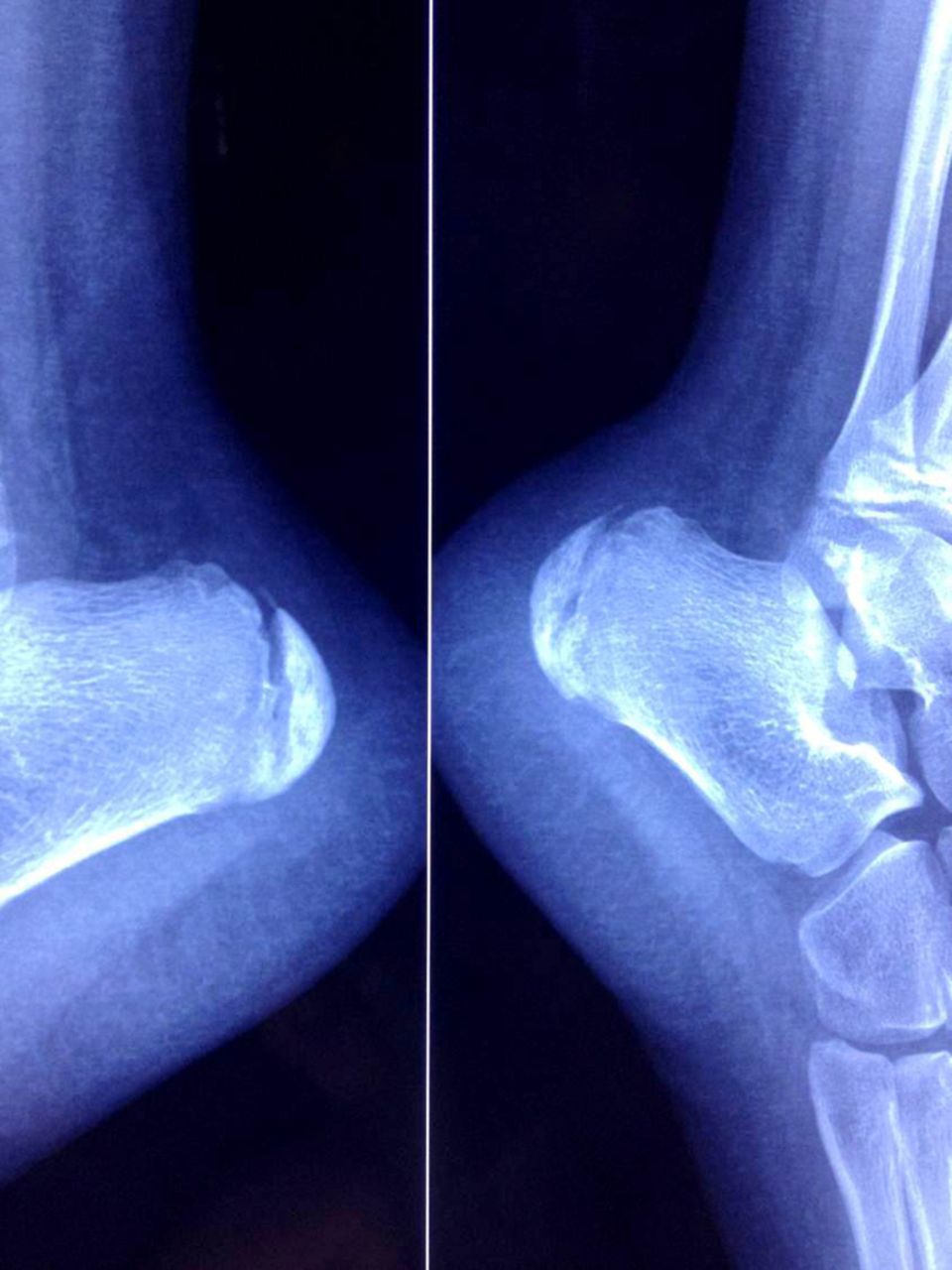
A 10-year-old boy presented with a 5 day history of refusal to walk due to severe bilateral heel pain, which increased with activity. The patient's family correlated the onset of pain to a preceding jumping activity by the child. There was no preceding history of rash, fever, respiratory tract or gastrointestinal tract symptoms. Examination revealed a well-nourished boy with normal vital signs. Foot examination revealed severe tenderness of lateral and posterior aspect of heel bilaterally. Other joint and systemic examination was normal. Laboratory tests showed white cell count 5×103/μl, haemoglobin 13.5 g/dl, platelet 215 × 103/μl, erythrocyte sedimentation rate 34 mm, C reactive protein 4.97 mg/dl and blood culture was negative. Rheumatoid factor, antinuclear antibody and anti-streptolysin O (ASO) titre levels were negative. Urine analysis, renal function, calcium level and chest x-ray were normal. Heel x-ray showed increased radiodensity of calaneal epiphysis with fragmentation on both sides (figure 1). MRI showed abnormal signal intensity of posterior calcaneal epiphysis and adjacent soft tissue (figure 2). He was given a course of oral and topical anti-inflammatory medication.

Heel x-ray showed increased radiodensity of calaneal epiphysis on both sides.

{kind=link}
{kind=link}
MRI showed abnormal signal intensity of posterior calcaneal epiphysis and adjacent soft tissue.
Sever disease (calcaneal apophysitis) is the most common aetiology of heel pain in growing children. It is postulated to be caused by repetitive microtrauma due to increased traction by Achilles tendon on its insertion site.1 Bilateral involvement is present in approximately 60% of cases.2 Plain x-ray of the heels would demonstrate sclerotic changes and fragmentation; however, this is usually difficult to distinguish from normal anatomic variation. MRI showed signal changes in posterior calcaneal epiphysis. Such cases are usually managed conservatively with anti-inflammatory medications and temporary cessation of physical activity.
Learning points
-
Sever disease is the most common cause of heel pain in growing children.
-
Bilateral calcaneal apophysitis may be seen.
-
It is usually managed conservatively with anti-inflammatory medications and restriction of physical activity.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed