Article Text

Statistics from Altmetric.com
Description
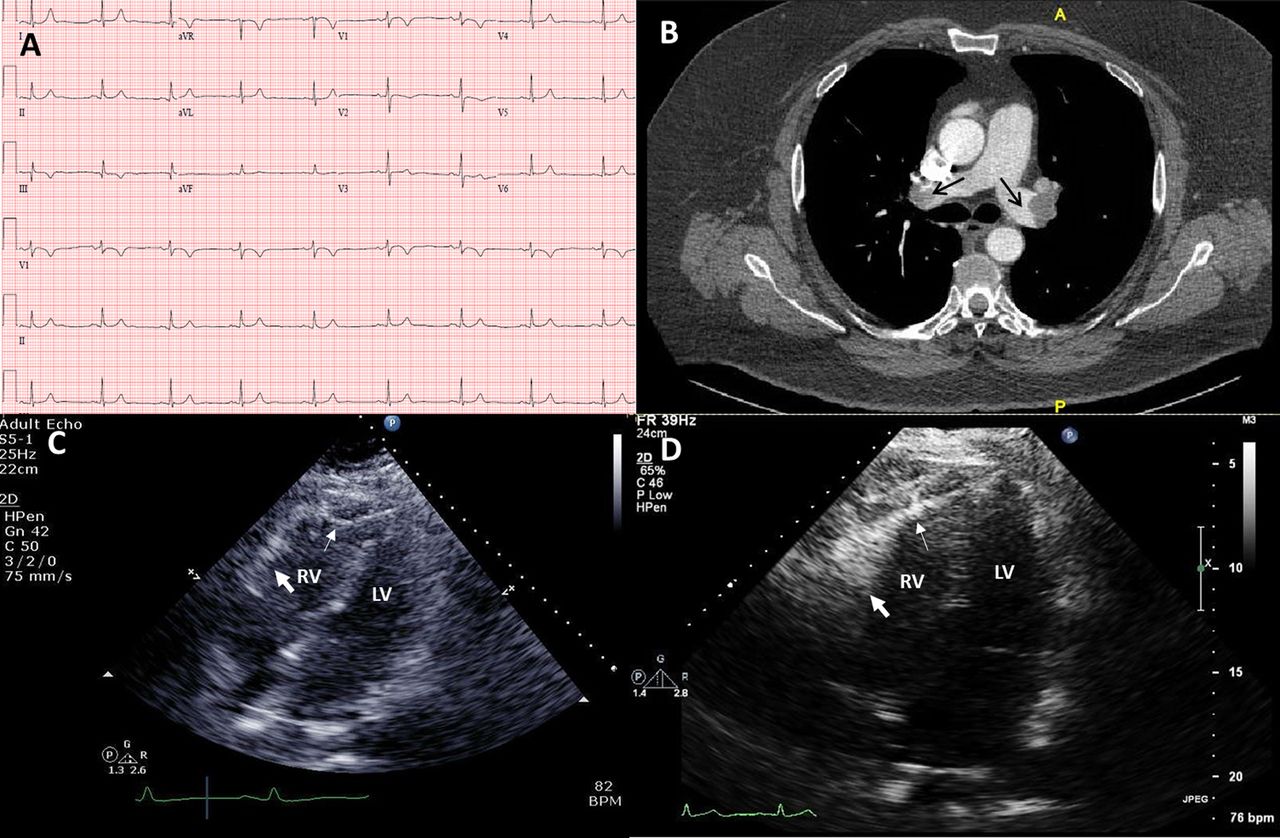
A 67-year-old man with a known history of venous thromboembolism was admitted with a 2 week history of dyspnoea. He denied chest pain, leg swelling or recent travelling. Clinical examination revealed blood pressure of 124/68 mm Hg, regular pulse of 54 bpm and respiratory rate of 27/min. Jugular veins were distended at 7 cm, and cardiopulmonary examination revealed no findings. ECG showed sinus bradycardia, S wave in lead I, Q wave in lead III with T-wave inversion (S1Q3T3) (figure 1A). Troponin T was negative and NT proBNP was elevated at 937 pg/ml. CT pulmonary angiography showed bilateral pulmonary embolism (figure 1B). Transthoracic echocardiogram revealed a moderately dilated right ventricle (RV) with moderate dysfunction. The RV apex was hyperkinetic and the free wall segment was akinetic, a finding consistent with McConnell sign (figure 1C). Anticoagulation was started, and the patient was discharged home in a stable condition. A repeat echocardiogram 2 months later showed disappearance of McConnell sign (figure 1D).1 ,2
{kind=link}
(A) 12-lead ECG showing sinus bradycardia, S wave in lead I, Q wave in lead III with T-wave inversion (S1Q3T3); (B) CT pulmonary angiogram showing large clots in right and left main pulmonary arteries (arrows); (C) apical-four-chamber view on transthoracic echocardiogram showing normokinesia of the right ventricular apical segment (thin arrow) and akinesia of the midfree wall (thick arrow). LV, left ventricle; RV, right ventricle; (D) apical-four-chamber view on transthoracic echocardiogram postanticoagulation showing resolution of right ventricular wall motion abnormalities. LV, left ventricle; RV, right ventricle.
Learning points
-
The role of transthoracic echocardiography in patients with pulmonary embolism is to evaluate haemodynamic stability, pulmonary hypertension and right ventricular (RV) strain.
-
The McConnell sign, identified as RV-free wall hypokinesia with hyperkinetic apex, is sensitive and specific in pulmonary embolism, and is associated with worse outcomes.
Footnotes
-
Contributors All authors have been involved in drafting the article and revising it critically for important intellectual content, and read and approved the final version of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.