Article Text

Summary
This article addresses issues related to pregnancy anaemia and late referral by a village birth attendant in resource poor setting in a central state of India. A young anaemic woman had labour onset at her village, a birth attendant tried to deliver her but failed. When she came to our hospital, had established septicaemia and absolutely non-reassurable uterine tone leading to intractable atonic postpartum haemorrhage. She died after 5 days because of coagulopathy and multiorgan failure. Huge budgets are being spent for the promotion of institutional deliveries but still the maternal mortality ratio has not reduced. The epidemiology of childbirth, social awareness for safe labour and administrative lethargy towards implementation of government programmes have not changed. The tertiary care—blood and components—multidisciplinary approach could not prevent the death of an anaemic woman. Unless there is a grassroot level change in the healthcare delivery system at the village level, the scenario might not change.
Statistics from Altmetric.com
Background
A 25-year-old woman was admitted to CR Gardi Hospital, a tertiary care institute located in Ujjain, India. The patient was in labour for more than 24 h. She landed in atonic postpartum haemorrhage (PPH) and succumbed to death despite blood and component transfusions and aggressive intensive care. Health facility at village and subsequent community health centre (CHC) had no emergency obstetric care (EmOC), forcing the patient to travel around 150 km to reach our hospital. The poor quality of woman reproductive healthcare in developing countries is a result of mishandled economy, corruption and illiteracy.1 Inadequacy of delivery care in remote areas in central state of India, Madhya Pradesh, is contextualised in this scenario. Those who do not have knowledge also do not have courage to accept it. The birth attendants in giving a trial of labour often waste precious time. In the present case not only 12-h period (of one night) was wasted in futile attempts to deliver but also, multiple internal examinations led to development of Gram-negative septicaemia superimposed on existing anaemia, resulting in massive atonic PPH and death. We aim to highlight epidemiological and health-system-related factors influencing maternal health in rural Madhya Pradesh, India.
Case presentation and treatment
Presenting features
A 25-year-old woman was admitted to obstetrics and gynaecology department of a 650-bedded university hospital in Ujjain, India. She gave a history of 9 months amenorrhoea, strong pain in the abdomen since last 24 h, along with ‘feeling of sinking’ and dizziness. She was a primigravida and did not know the date of her last menstrual period. History revealed she had taken two injections of tetanus toxoid in the village and some iron and folic acid tablets. She did not receive any other obstetric care. She belonged to a village located in a neighbouring district, 150 km away from our hospital. The occupation of the family is farming. Income of her family is around 5000 rupees (approximately US$100) per month. There was no relevant feature in family history.
Health systems background and prereferral care
The village to which the patient belonged has a population of 950 and has no healthcare facility. There is a CHC, located 20 km away from her village. The village is connected to this CHC with a kachha (non-tar) road. At the CHC, two qualified primary care physicians are available for daytime outpatient care and two-auxilliary nurse midwives (ANM) stay round the clock for labour cases. However, CHC is not a facility, thus all complicated obstetric cases are referred out. Our patient revealed the history of having onset of abdominal pain since last morning and she stayed at home waiting for her delivery. In the night at 23:00 she was taken to the CHC, where the ANM gave her some intravenous fluids. Multiple vaginal examinations were carried out. In the morning as there was no progress of labour she was asked to go to our hospital and she reached at 12:15 the next day.
Clinical findings and treatment
On admission, that is, at zero hour, the young patient was dehydrated, with sunken eyes and in agony. Blood pressure (BP) was 106/80 mm Hg and pulse rate 100/min. The core temperature was 38.4° C but the peripheries were cold on touch. She looked pale and toxic. Uterus was full term with strong uterine contractions and head was engaged, fetal heart sound was absent. Vaginal examination revealed fully dilated cervix, 1 cm caput and head at plus one station. Examination of other systems revealed no abnormal signs. Her haemoglobin (Hb%) was 5 g/dL, total leucocyte count 20 000/mm3 and platelet 1 43 000/mm3. We decided to deliver the patient by low forceps under intravenous sedation. It was an easy outlet forceps delivery. A stillborn baby was delivered. There was no moulding of the head of stillborn baby. After placental delivery of the patient started bleeding per vagina and the uterus was found to be flabby and atonic. She was given intravenous crystalloids with 40 units oxytocin infusion, and manual uterine massage. However, she still continued to bleed; intravenous carboprost 250 µg and per rectal misoprostol 800 µg was also given. Simultaneously, the vagina and cervix was explored and no tear was found. By end of first hour, the patient lost about 600–800 mL blood and was started infusion of red blood cell concentrate (RBC) according to guidelines.2
By the second hour bleeding still continued profusely and we proceeded for obstetric hysterectomy. In our setting uterine artery embolisation is not routinely performed and we were not sure of immediate cessation of bleeding after ligation of internal iliac vessels. On opening the abdomen the uterus was absolutely pale, white and revealed no injury (figure 1). The patient was shifted to intensive care unit at end of 2.5 h of admission with systolic BP at 80 mm Hg and tachypnoea. The patient was put on ventilator support.

Intraoperative photograph of a pale white uterus in massive atonic postpartum haemorrhage.
At the end of sixth hour central venous pressure (CVP) was 5 cm, platelet count 40 000/mm3 and the patient was in haemorrhagic shock. In view of her clinical condition RBC concentrates continued to be replaced and she was started on dopamine infusion. Her prothrombim time was 14 s and activated partial thromboplastin time 45 s. Coagulation profile and haematological parameters are shown in table 1 in consecutive order.
Details of haematological and serological investigations along with transfusions given
To summarise in the first 24 h of admission, the patient had lost about 3–4 L blood because of atonic PPH. Her CVP was going down, Hb was low and general condition was poor. Urine output was adequate throughout and remained proportionate to input till day 5. On day 1 the abdomen was mildly distended, with pelvic ultrasound showing about 400 mL collection. She was given blood and components, antibiotics–imipenem and metronidazole; intravenous tranexamic acid 2 g/day with high-dose hydrocortisone.
On day 2, abdominal and pelvic collection increased, basal effusions in lung appeared and pallor increased. With a suspicion of active bleeder, we carried out exploratory laparotomy. It revealed about 1000 mL clot on the vault of vagina and about 3 L free blood. Haematoma was drained and bilateral internal iliac artery ligation was carried out.
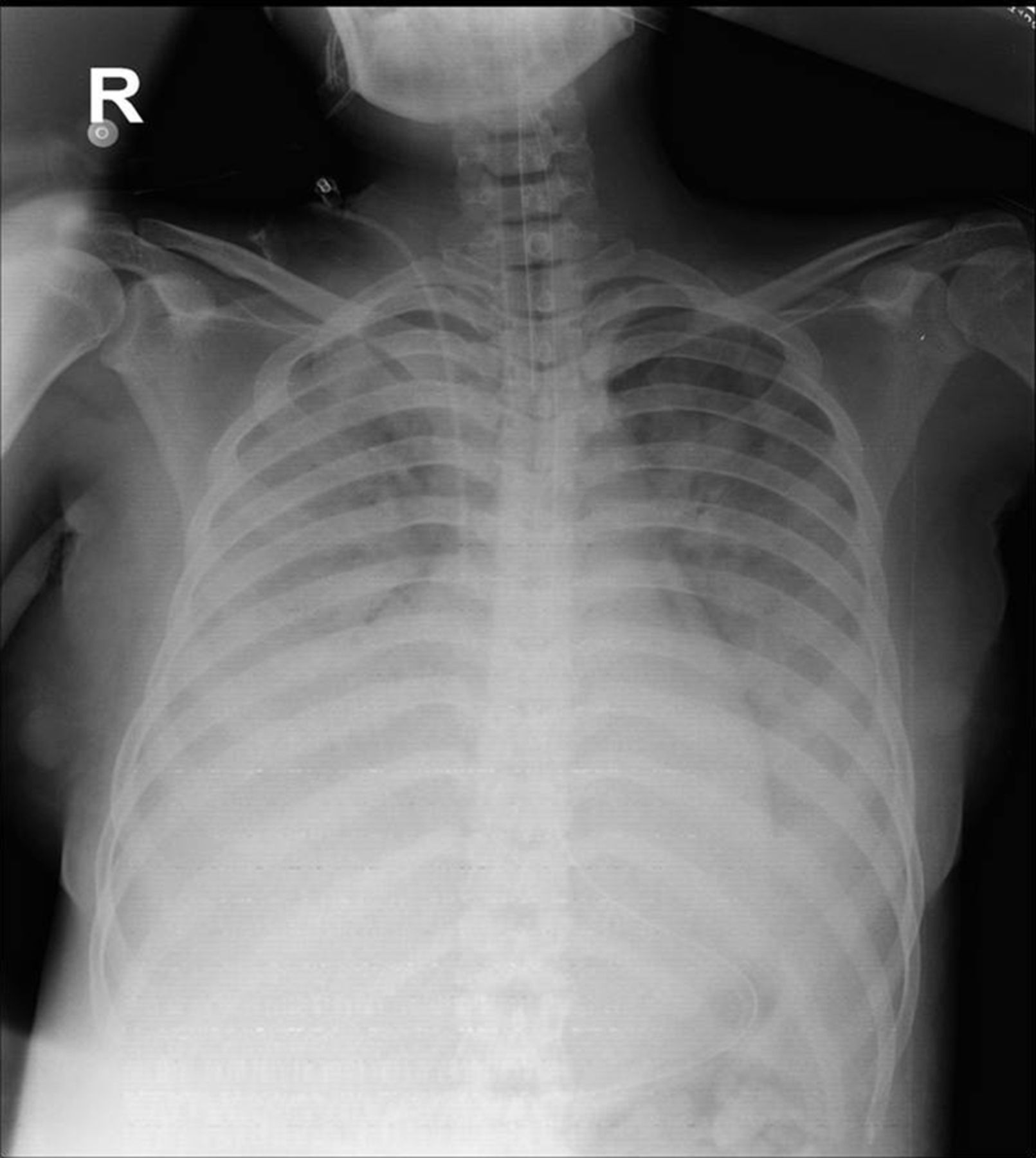
On day 3, the patient's level of consciousness improved. She was given epsilon aminocaproic acid (200 mg intravenous). On day 4, tachypnoea was seen and basal crepitation in lung appeared. Her Hb was 9 g/dL. Considering fluid overload we treated her with intravenous frusemide-200 mg (divided doses), but without response. On day 5, she had a clinical picture of non-cardiogenic pulmonary oedema (figure 2). The ventilator tubing was repeatedly filled with pink coloured froth. The patient succumbed on the night of day 5.
{kind=link}
{kind=link}
X-ray chest showing fluffy white lung shadows involving whole of lungs in advanced pulmonary oedema.
Investigations
See table 1.
Differential diagnosis
-
Traumatic PPH
-
Atonic PPH
Outcome and follow-up
The patient died of acute non-cardiogenic pulmonary oedema following multiorgan failure secondary to atonic PPH and subsequent coagulopathy causing haemorrhagic shock.
Discussion
The major factors causing this death are antecedent anaemia and intractable atonic postpartum haemorrhage. Anaemia is directly or indirectly responsible for 40% maternal deaths. There is a 8–10-fold increase in maternal mortality ratio (MMR) when Hb falls below 5 g/dL.3 Anaemia, which was present in this patient, caused a weak and non-reassureable uterine tone4 Anaemia causes rise in nitric oxide levels, which is responsible for hypotonic myometrium in atonic PPH.4 In the Indian context, haemorrhage is the chief cause of maternal deaths, that is, 31%.5 The present case was managed in a tertiary care hospital with the best of facilities. Ventilator support and massive blood transfusions could not save this patient; neither the timely administration of high concentration of oxytocin infusion nor carboprost and rectal misoprostol.6–8
The Government of India has started a cash incentive scheme—Janani Suraksha Yojna —to promote institutional deliveries with an aim to reduce MMR since year 2005. As such the rate of institutional deliveries has increased.9–11 Still the question is why the MMR has not gone down? In another district in Madhya Pradesh, following local protests against a high number of maternal deaths in 2010, a study was carried out to find out causes of 27 maternal deaths.12 The study revealed absence of antenatal care despite high levels of anaemia, absence of skilled birth attendants, failure to carry out emergency obstetric care and referrals that never resulted in treatment contributing to maternal deaths.12 Most of the above causes are substantiated by our case as well. We do not have significant epidemiological data of outcome and complications of the women referred from rural areas to Ujjain district; however, a project is ongoing which will provide this much needed information in future.11
A few studies suggest an increasing trend for this sudden, unpredictable, life-threatening condition, that is, atonic PPH. A recent study from Vancouver, Canada observed an increase in atonic PPH, from 4.8% in 2001 to 6.3% in 2009.13 This increase was not related to labour induction, augmentation or caesarean delivery.13 An Irish study14 also revealed a threefold increase of atonic PPH between 1999 and 2009. The study highlighted the pressing need for research and for clinical audit focusing on aetiological factors, preventative measures and quality of care, to guide current clinical practice.14 Biological differences may also play a role. Hispanic ethnicity and Asian/Pacific Islander race are significant risk factors for atonic PPH independent of measured potential mediators.15 Ethnicity may also play a role in the present case. In conclusion, we feel there is an unanswered question as to what was behind this sudden and massive PPH which killed a young woman. Of course, the prevailing anaemia and poor obstetric care prior to admission contributed to the outcome.
Learning points
-
Anticipate atonic uterus and septicaemia in anaemic patient referred from periphery with prolonged labour.4
-
Haemostatic resuscitation in form of tranexamic acid, blood components and early intensive care with ventilator support are components of good patient care.
-
MSBOS (maximum surgical blood ordering schedule)2 should be followed for obstetric patients with haemoglobin (Hb)<7 g, requiring general anaesthesia, in major blood letting surgery and symptomatic anaemia regardless of haemoglobin level.
-
Minutes count in atonic postpartum haemorrhage; quick and aggressive decision-making is key to saving the patient's life.
-
Tertiary care alone will not reduce maternal mortality ratio but a social drive that respects the quality of care received at delivery is also needed.
Acknowledgments
The authors thank the medical director Dr VK Mahadik and Dean, Dr JK Sharma, RD Gardi Medical College, Ujjain for granting us permission to publish this case.
Footnotes
-
Contributors KM, MBS and NP collected the clinical details and photographs of the patient's report. KM performed the literature review and drafted the manuscript. KM verified the diagnosis and other scientific facts. KM, MBS, NP and AP revised the manuscript critically for substantial neurological content. All authors read and approved the final manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.