Article Text

Statistics from Altmetric.com
Description
A 46-year-old non-smoking, mildly asthmatic woman presented with a 2 -day history of breathlessness and cough. Examination revealed a tachypnoea and bilateral expiratory wheeze. Arterial blood gas analysis showed a type 1 respiratory failure, chest x-ray showed patchy consolidation at the right base.
She was treated for exacerbation of asthma and right-sided pneumonia.
The patient subsequently developed worsening respiratory failure, was intubated and taken to intensive care unit.
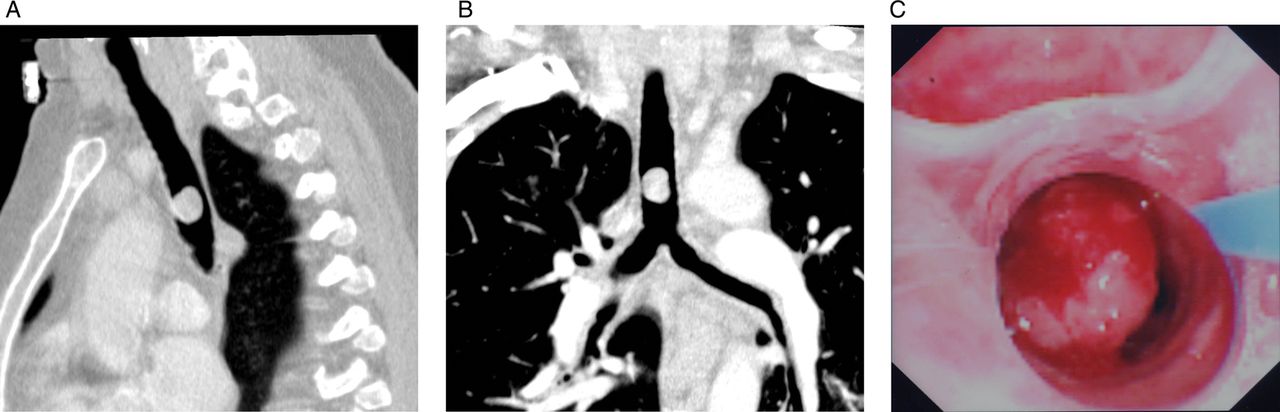
After a short period of intubation, she was extubated and had severe coughing and haemoptysis. Suspecting pulmonary embolism a CT pulmonary angiogram was undertaken which showed a mass in the trachea (figure 1A,B). After re-intubation, bronchoscopy revealed a pulsatile mass in the lower third of the trachea, this occupied approximately 80% of the tracheal diameter (figure 1C).

{kind=link}
(A) CT sagittal section of thorax (B) CT coronal section of thorax both (A) and (B) show a foreign body occupying the trachea above the carina. (C) Broncoscopy of the lower third of the trachea demonstrating the occluding neoplasm, brushings were taken on direct visualisation for histology.
She was transferred to a specialist centre, where she underwent cryotherapy. The histology was adenocarcinoma. She has been referred to the oncologists for chemotherapy.
Primary tumours of the trachea account for less than 0.1% of all tumours and are commonly misdiagnosed as asthma or chronic lung disease.1
Squamous cell carcinoma and adenoid cystic carcinoma being the most common histological diagnosis for primary airway neoplasms accounting for two-thirds of all tracheal malignancy.2 CT is the most useful imaging modality, allowing visualisation of tumour and any invasion into surrounding structures. Thereafter bronchoscopy allows for tissue diagnosis and for assessment of surgical resectability of such a lesion.3
Learning points
-
Wheeze is characteristically heard in abnormally narrow or compressed airways, asthmatic wheeze will typically respond to asthma exacerbation therapy; where wheeze is difficult to break consider differentials.
-
CT imaging and bronchoscopy can be useful in staging of neoplasms of the upper airways.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.