Article Text

Statistics from Altmetric.com
Description
A lady in her 50s was transferred to the neurosurgical department with reduced conscious level resulting from subarachnoid haemorrhage. The culpable anterior communicating artery aneurysm was coiled without complication.
The following day she remained drowsy and slightly dysphasic, but intimated a sudden alteration in visual acuity in her right eye. On examination, she was unable to count fingers in the right eye and struggled to see the light of the pen-torch. Right-sided relative afferent pupillary defect was present. No other cranial nerve abnormalities were detected.
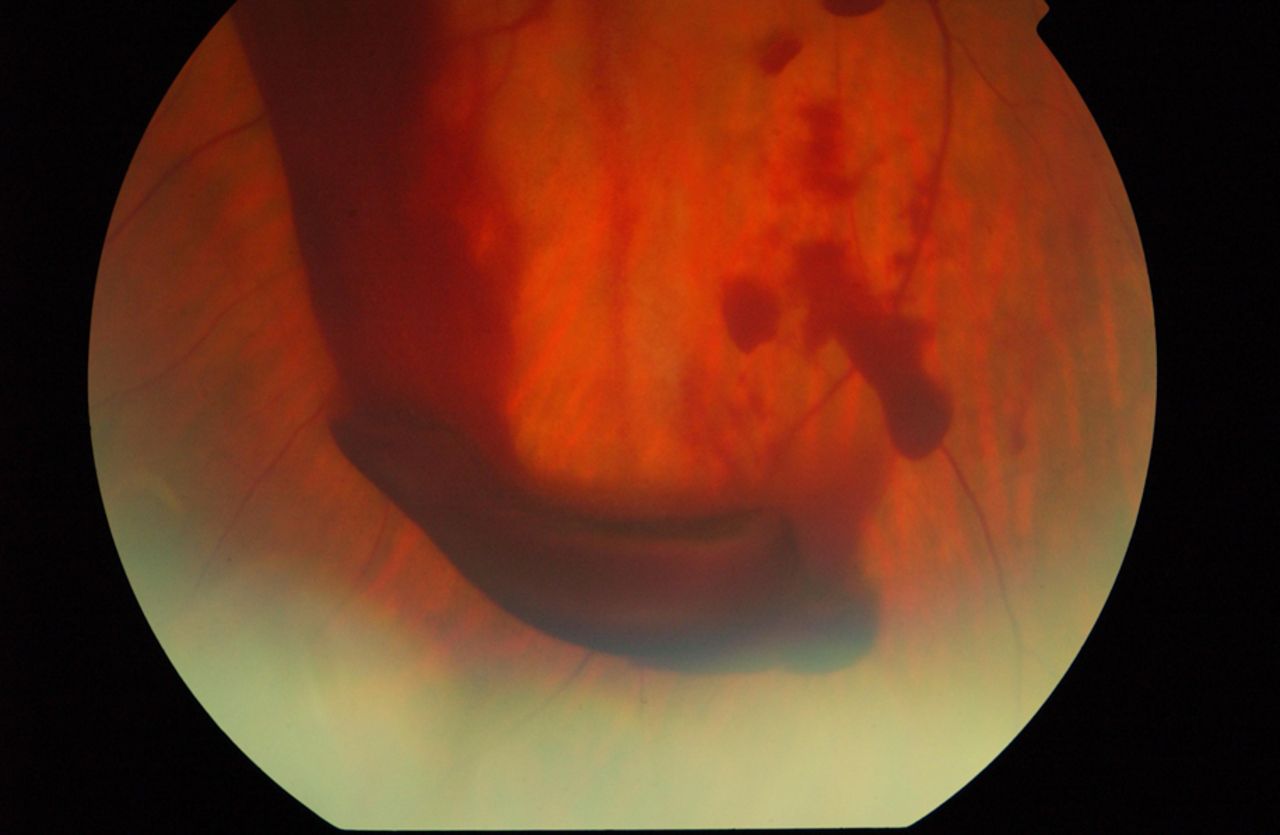
Upon examination of her right fundus copious intraretinal and subhyaloid haemorrhage was seen involving the macula area (figures 1 and 2). The left fundus showed some small haemorrhages but visual acuity was unaffected.

Right fundus showing copious intraretinal and subhyaloid haemorrhages involving the macula area.

{kind=link}
{kind=link}
Right fundus showing copious intraretinal and subhyaloid haemorrhages.
The French Ophthalmologist Albert Terson is credited with recognising intraocular haemorrhage occurring in conjunction with subarachnoid haemorrhage; Terson's syndrome.1 One systematic review found Vitreous, retinal or subhyaloid haemorrhage to occur in 13% of patients with subarachnoid haemorrhage.2 The pathological mechanism remains unclear although it is thought that raised intracranial pressure forces blood into the subarachnoid space, along the optic nerve sheath and into the preretinal space. The sudden rise in intracranial pressure may also lead to a decrease in venous return to the cavernous sinus or obstruct the retinochoroidal anastomoses and central retinal vein, resulting in venous stasis and haemorrhage.
Spontaneously clearing vitreous or intraocular haemorrhage is most common. Elevated head positioning with bed rest and witholding anticoagulant medications is important. Larger haemorrhages may require vitrectomy to aid resolution, especially if both eyes are involved.
Learning points
-
Terson's syndrome is an uncommon but potentially sight threatening complication of subarachnoid haemorrhage.
-
Fundal examination is essential in all patients presenting with Subarachnoid haemorrhage.
-
Ophthalmic referral is necessary in all patients with decreased visual acuity as surgical intervention may be required.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.