Article Text

Summary
This report describes a 10-month-old infant who presented with generalised tonic clonic seizures following 2 days of vomiting, diarrhoea and a low-grade fever. The patient was moderately dehydrated and the blood investigations were remarkable for hyponatraemia (126 mEq/l), leukocytosis (19.4 × 103/l (46% lymphocytes)), thrombocytosis (637 × 103/l), hypoalbuminaemia (albumin 1.9 g/dl) and elevated C reactive protein (96 mg/l). Stool was positive for white and red blood cells but the cultures for bacteria were negative. Rotavirus antigen in stool was positive. There was microscopic haematuria without proteinuria and the nasogastric aspirate was coffee ground. Generalised oedema with pleural and peritoneal effusions ensued requiring drainage, correction of fluid and electrolytes imbalance and albumin infusions. Over the next 72 h, the patient descended into shock and disseminated intravascular coagulopathy which required packed red blood cells and fresh frozen plasma transfusions. By day 12 the patient was clinically and biochemically normal.
Statistics from Altmetric.com
Background
Rotavirus is the most frequent cause of childhood diarrhoea worldwide. While the rotavirus vaccines have recently made some headway, the international burden keeps shifting to the low to mid-income countries where it remains the leading cause of infant mortality.1 Rotavirus typically affects infants, who characteristically present to the hospital emergency with low-grade fever, vomiting and watery stools with mild to moderate dehydration. Providing electrolytes and water replacement while resuming the child’s feeding remain the main objectives of the care givers. Some children are admitted if they do not tolerate oral rehydration therapy. The diagnosis is often confirmed with the stool enzyme immunoassay (EIA) for rotavirus antigen and helps isolate the cases when admitted to the hospital to limit nosocomial transmission. Extraintestinal complications of rotavirus infection have been said to occur rarely2 3 and often lead to higher morbidity and mortality. Rotavirus-induced central nervous system (CNS) involvement has been associated with seizure, encephalopathy and death.4 Likewise shock and disseminated intravascular coagulation (DIC) are rare but potentially lethal5 complications associated with the rotavirus infection.6 In an 11-year surveillance study conducted in a Swedish population, rotavirus infection attributed complications occurred in 16.5% of children with community acquired rotavirus gastroenteritis and 1.9% of nosocomial acquired rota infection. These complications consisted of severe dehydration resulting in intensive care (1.7%), death (0.1%), hypertonic dehydration (9.1%), seizures (4.0%) and encephalitis with abnormal EEG (1.7%).3 This case report emphasises the importance of recognising the rare but serious complications of a common enteric pathogen. The course of illness points to the versatility of the virus in altering the course of an otherwise benign gastroenteritis.
Case presentation
A previously healthy 10-month-old female infant presented to a hospital emergency room (ER) with two brief (5 min) and consecutive episodes of generalised tonic clonic convulsions after a 2-day bout of vomiting, diarrhoea and low-grade fever. Upon arrival to ER, her blood pressure was 102/54 mm Hg, heart rate was 150 beats/min, respiratory rate was 34 breaths/min, body temperature was 37.8°C and oxygen saturation was 94% on room air. She was lethargic and had dry mucous membranes. The anterior fontanelle was depressed and the capillary refill was delayed (3 s).The pupils were equal and reactive to light with normal fundoscopic examination and there was no neck stiffness. Random blood sugar was 121 mg/dl. After initial stabilisation (hydration, correction of electrolyte imbalances and seizure control), CT of the brain was done and reported as normal. The blood tests revealed hyponatraemia (Na 126 mEq/l), hypoproteinaemia (total protein 4.2 g/dl, albumin 1.9 g/dl), and leukocytosis (white blood cell (WBC) 19.4 × 103/l (46% lymphocytes)), thrombocytosis (637 × 103/l) and elevated C reactive protein (CRP, 96 mg/l). Urine was positive for blood (red blood cell (RBC) 30/106). Blood, urine and cerebrospinal fluid (CSF) were sent for culture and broad spectrum antibiotics – ceftriaxone and vancomycin – were administered intravenously empirically for sepsis.7 Intravenous albumin infusions were also started at this time followed by a loop diuretic as needed.
Over the next 24 h, the patient developed generalised oedema with ascites and pleural effusion. Due to the laboured breathing, dyspnoea, hyperpnoea and continued acidosis, the patient was transferred to the intensive care unit where parecentesis and thoracocentesis were performed and a chest tube was left in place to drain. Endotracheal intubation was not needed. Stool was positive for RBC and WBC but the gram stain was negative. Stool EIA was however positive for rotavirus antigen. Cultures of urine, stool, blood and cerebrospinal fluid (unremarkable chemistry-protein, glucose and cell count within normal limits) were reported negative for bacterial and fungal growth.
On day 4 post admission, low-dose intravenous methylprednisolone was started due to persistent hypoalbuminaemia, increased oxygen requirements and risk of septic shock.8 On day 6, the patient became tachycardiac and hypotensive and the blood results showed neutropaenia (WBC 3.25 × 103), thrombocytopaenia (82 × 103), anaemia (haemoglobin 8 g/dl) and coagulopathy (D-dimer elevated to 2055 ug/l, prothrombin time rose to 16 s and partial prothrombin time went up to 53 s). Intravenous ceftazidime was substituted for ceftriaxone to broaden the coverage to include Pseudomonas aeruginosa. The patient received fresh frozen plasma (FFP) and packed red blood cells (PRBC) transfusions.
The cultures from the pleural and peritoneal effusions (transudate) were negative for bacterial and fungal growth. Endoscopy and colonoscopy were visually normal. The duodenal biopsies showed some patchy areas of short and broad villi and diffuse oedema but no significant inflammation/ulceration or mucosal damage (figure 1). Gastric and oesophageal biopsies were normal. Colonic mucosa was mildly oedematous with no significant inflammation (figure 2). The patient showed complete clinical and biochemical recovery 12 days after the hospital admission (figures 3–5) and remained well upon her follow-up outpatient visit 2 months later.
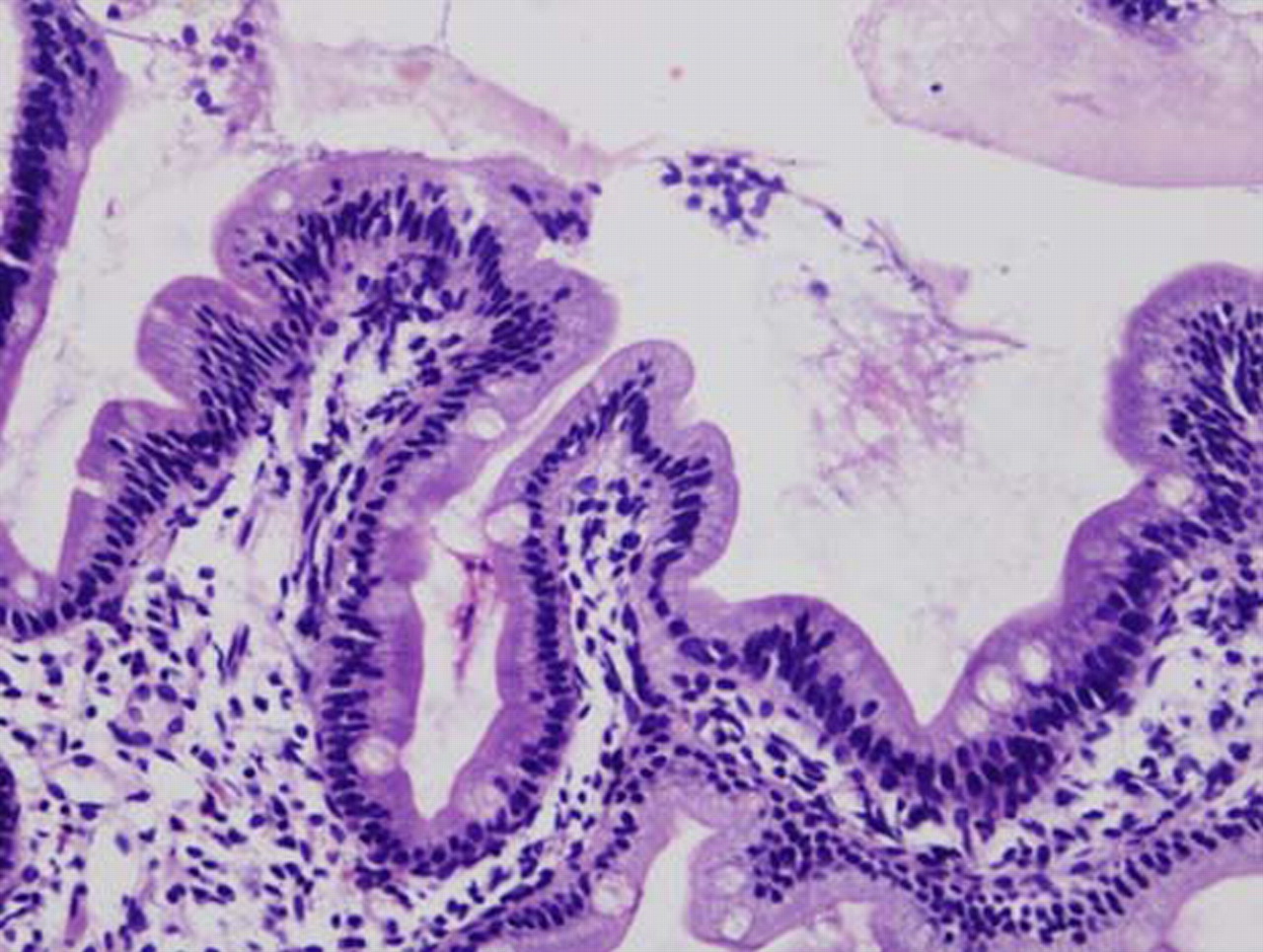
Villous blunting in the duodenal biopsy sample (400 ×).

Mild oedema in colon biopsy sample (400 ×).
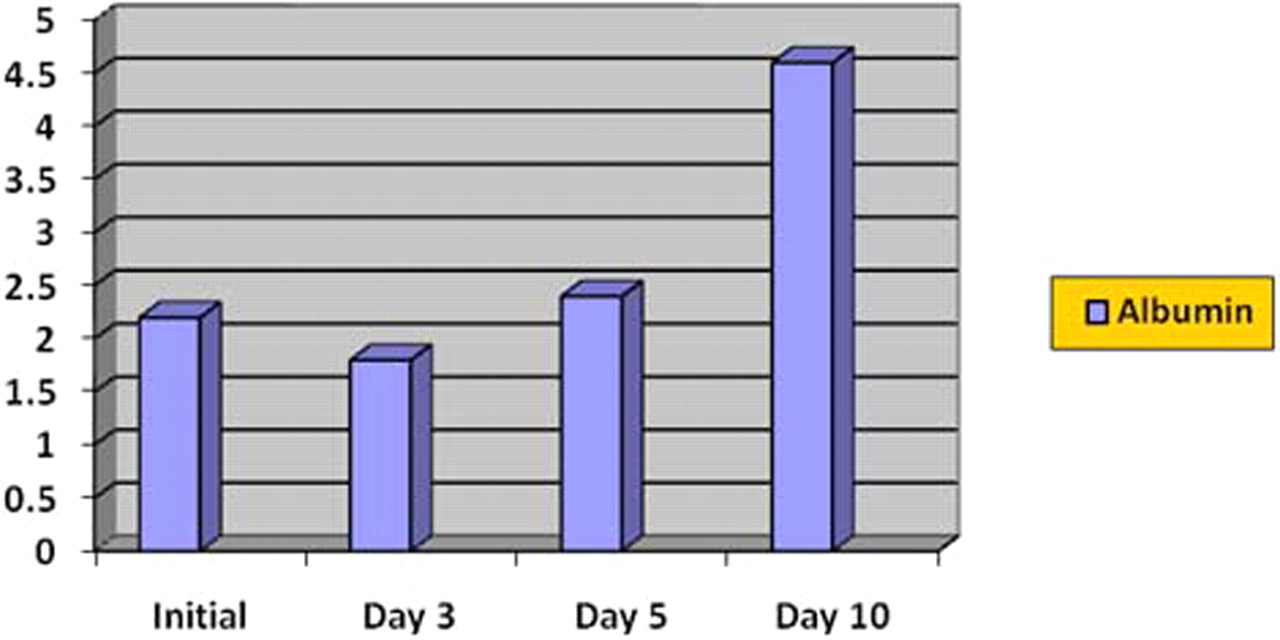
Serum albumin level from day 0, 3, 5 and 10.

Blood platelet count (× 103) on day 0, 5, 7, 10 and 13.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
D-dimer assay in ug/l on day 7, 10 and 13.
Investigations
▶ Stool RIA was positive for rotavirus antigen but bacterial cultures were negative
▶ Initial blood tests indicated elevated CRP, hyponatraemia and hypoproteinaemia
▶ Blood tests on day 6 revealed a DIC like picture
▶ Random blood glucose was normal
▶ CT scan of the brain and EEG was reported to be normal
▶ Duodenal biopsy showed patchy areas of broad and flattened villi and oedema.
Differential diagnosis
▶ Extraintestinal complications of ROTA virus gastroenteritis
▶ Unidentified bacterial sepsis, shock and DIC.
Treatment
Correction of fluid and electrolyte imbalance, albumin, FFP and PRBC transfusions, pleural tap and peritoneal drainage and nutrition support.
Outcome and follow-up
Complete clinical and biochemical recovery.
Discussion
Although plausible by deductive reasoning from the literature,9 elevated CRP attributed to rota virus gastroenteritis without concomitant bacteraemia or bacterial infection has never been reported. Systemic inflammatory response syndrome (SIRS) can occur with viral infections and has been described due to norovirus, rotavirus and astrovirus in the neonates.10 Rotavirus associated seizures and encephalopathy11 4 as well as protein loosing enteropathy12 and shock6 13are less recognised and much less understood manifestations. Although two cases of DIC associated with rotavirus have been reported, it is difficult to undermine the contribution of hypovolemic shock and metabolic derangements in those cases.13 Moreover, CRP was not measured in either of them and neither of them had undergone colonoscopy to rule out colonic injury for certain. The case underscores our limited understanding of the alterations in the host immunity behind these unusual presentations of a common enterovirus infection.
This is an infant with rotavirus gastroenteritis and sepsis (SIRS with infection or suspected infection), and negative blood, urine, stool and CSF cultures. Seizures, protein loosing enteropathy and DIC as complications of rotavirus infection are rare individual events and the combination in a single patient, not documented in recent literature. Elevated CRP (>80 mg/l) occurs in 5% of viral infections,9 but has never been reported with rotavirus infection. The diagnosis in this case was based on rotavirus antigen identified in the stool of the patient upon initial presentation. Had we not sent the stool for the RIA on day 1, or had we sent it later during the hospitalisation, the case would have either remained hitherto riddled in the former scenario or labelled nosocomial in the case of the latter. In any event we would have exposed other hospitalised children to rotavirus infection.
Learning points
▶ Diagnosis of rotavirus is very important in sick children who need hospital admissions in order to isolate and prevent nosocomial outbreaks.
▶ CRP could be elevated in rotavirus infection without bacteraemia.
▶ The CNS complications of rotavirus can be fatal and hyponatraemic seizures can be an initial presentation.
▶ Rapid fluid shifts, hypoproteinaemia, DIC and SIRS can occur with rotavirus gastroenteritis.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.