Article Text

Statistics from Altmetric.com
Description
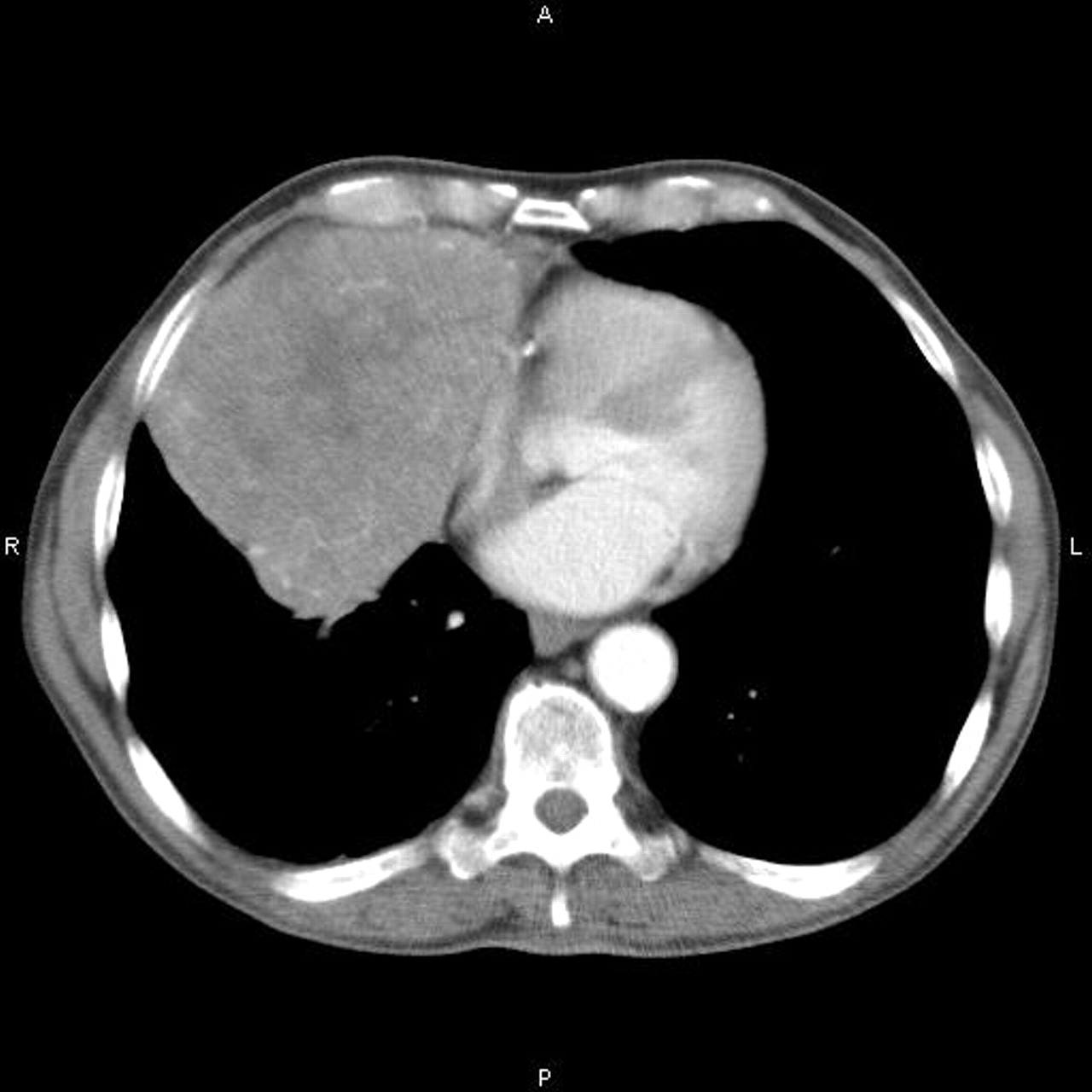
A 76-year-old patient presented with an incidental finding of an anterior mediastinal mass (figures 1 and 2) following investigations for pneumonia. The patient underwent median sternotomy and excision of the mass. The mass weighed 1 kg and measured 15×14×10 cm. Histology revealed a grade AB thymoma of Masaoka stage II due to microscopic capsular invasion (figure 3). The patient made an uneventful postoperative recovery.

Chest x-ray showing mediastinal mass.

CT showing anterior mediastinal mass.

Lymphoid cells (black arrow) and spindle shaped epithelial cells (red arrow) indicating the two cellular components in AB thymoma.
Thymoma is the most common tumour of the anterior mediastinum with an incidence of 0.10–0.18 per 100 000. Overall, 35–50% of patients with thymomas have myasthenia gravis, while 12% of patients with myasthenia gravis have a thymoma. Approximately 50% of individuals presenting with thymomas are clinically asymptomatic. Symptoms include chest pain, cough, dyspnoea and muscle fatigue (characteristic of myasthenia gravis). Less common symptoms, such as superior vena cava syndrome, phrenic nerve paralysis or recurrent laryngeal nerve involvement resulting in hoarseness, are indicative of malignant disease. The differential diagnoses of anterior mediastinal masses include lymphoma, retrosternal thyroid and germ cell tumours.
Patients with a suspected mediastinal mass as suggested in figure 1 should undergo CT scan. There were no features to suggest invasion into surrounding structures (figure 2) and in such cases complete surgical resection should be attempted (figure 4). Grade A or AB tumours of Masaoka stage I or II do not require adjuvant treatment.1 2 However, neoadjuvant therapy should be considered for patients with large or invasive tumours. Surgical resection or debulking with adjuvant chemo-radiotherapy reduces the risk of recurrence in those with stage III (local invasion) or stage IV (distant metastases) disease.3 Predictors of long-term survival include complete surgical resection, stage, histological grade and size of tumour. Intra-thoracic recurrence is more likely in advanced stages but overall cause of death is unrelated to thymoma in 65% of patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Thymoma completely excised.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.