Article Text

Summary
The presentation of intracerebral tumours with tremor is rare. A case is described of a 78-year-old woman presenting with Holmes’ tremor who was found to have a thalamic tumour. The diagnostic context of tumours that present with tremor is discussed along with the pathophysiology and management of this case.
Statistics from Altmetric.com
Background
Intracerebral tumours rarely present with an isolated tremor. This case is unique as the primary manifestation of this thalamic tumour was a slowly progressive tremor of the Holmes’ variety which is present at rest and worsens with movement.1 Isolated cases of other thalamic lesions presenting only with Holmes’ tremor have also been reported but not specifically from a thalamic tumour.2–4 Tumours presenting with parkinsonian and cerebellar tremors have been described but these are associated with other symptoms and signs.5 The diagnostic uncertainty that resulted from an unusual presentation is described along with subsequent management options.
Case presentation
A 78-year-old left handed woman presented with a 7 year history of left upper limb tremor. The tremor was of insidious onset with progressively increasing frequency and intensity. It was present at rest and during activities, causing her to spill drinks. Propanolol had had no benefit. The patient also suffered from chronic intermittent bilateral occipital headaches which improved with aspirin. Two previous computed tomography (CT) scans for headache reported a small old infarct in the right thalamus. The patient was hypothyroid and on thyroxine, and was a smoker of 20 pack years. Her mother also suffered a tremor of unknown character.
On examination the patient had an obvious upper extremity left sided tremor at rest. The tremor had a frequency of 5 Hz and increased in amplitude on both postural and intention testing. Cranial nerves were intact. A localised patch of numbness to light touch was noted on the lateral aspect of the left forearm and hand. Otherwise, tone, power, reflexes and sensation were normal in the upper and lower limbs with no signs of Parkinsonism.
Investigations
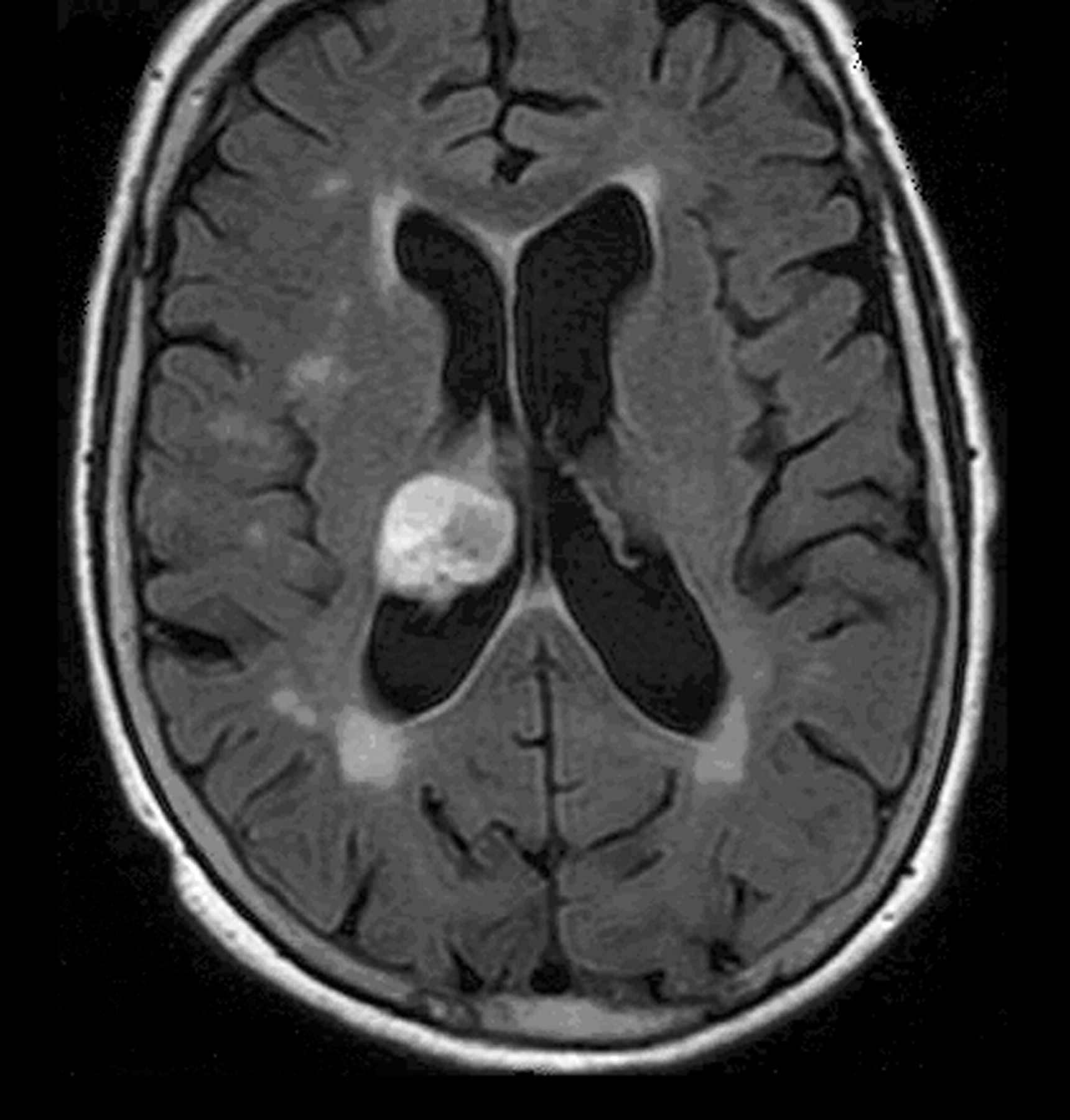
Routine laboratory blood tests were normal. Magnetic resonance imaging (MRI) of the brain demonstrated a well circumscribed 2.5×3×2.3 cm mass occupying most of the right thalamus and projecting exophytically into the right lateral ventricle and third ventricle. It was heterogeneously hyperintense on fluid attenuated inversion recovery (FLAIR) sequence (fig 1) and hypointense on T1 sequences. No diffusion restriction, oedema, haemorrhage or gadolinium enhancement was present. The possibility of metastatic disease was ruled out by further investigations including CT of the chest, abdomen and pelvis.

{kind=link}
Fluid attenuated inversion recovery (FLAIR) sequence magnetic resonance image demonstrating heterogeneously hyperintense thalamic mass projecting into the lateral ventricle.
Differential diagnosis
Before imaging the presence of an isolated Holmes’ tremor localises pathology to either the midbrain or thalamus with documented pathologies including tumours, abscess, cerebrovascular lesions and multiple sclerosis.6–9 In this case, the MRI clearly demonstrated a well defined mass lesion. With no diffusion restriction or gadolinium enhancement this is thought to most likely represent a low grade glioma or ependymoma rather than an abscess or high grade tumour.
Treatment
Given the size and location of the tumour, and the patient’s reasonable functional status, surgical intervention was not advised.
Outcome and follow-up
The patient was advised to return to clinic in 6 months time with further imaging to review the lesion.
Discussion
This is a rare presentation of a thalamic tumour solely with tremor. A case series of 225 patients with astrocytomas of the basal ganglia or thalamus described tremor in 12 patients, six of whom suffered a Holmes’ tremor.2 Although initial presentation is not published, all these patients had other symptoms or signs at the time of biopsy. Thalamomesencephalic cavernomas and ependymal cysts have been reported presenting as parkinsonian or Holmes’ tremor,3 and a case series of bilateral thalamic tumours in children reports one case presenting with unilateral intention and rest tremor.4 Other tumours that present with tremor include those presenting with unilateral resting tremor and subsequently parkinsonism which are usually extra-axial, although intra-axial tumours usually distant from the basal ganglia have also been reported.5 Posterior fossa masses can present with intention tremor although other cerebellar signs and symptoms are usually present. It is therefore important to consider intracranial tumours in a patient presenting with unexplained tremor. In this case the diagnosis was masked by a thalamic infarct, but the diagnosis of an underlying tumour might have been considered on the basis of progressive symptomatology.
The Holmes’ tremor, also known as rubral or midbrain tremor, was first described by Gordon Holmes in 1904.1 It is characterised by a 2–5 Hz, upper extremity tremor present at rest and exacerbated by posture or movement. Most commonly this tremor is associated with pathology of the upper brainstem including tumours, vascular insults and multiple sclerosis.6,7 Pathology in the thalamus is a less common cause although tumours, cysts, vascular insults and abscesses leading to Holmes’ tremor have been described.4,8,9 The tremor is believed to result from disruption of the dentate–rubro–olivary and cerebello–thalamo–cortical pathways. Concurrent lesion of nigrostriatal pathways is postulated to cause the resting component which may respond to levodopa and dopamine agonist pharmacotherapy.10
Tumours of the thalamus may be treated by surgical resection, fractionated radiotherapy, stereotactic radiosurgery for smaller low grade tumours, and more recently endoscopic management.11 Gross total resection can be successful with long term survival and acceptable morbidity, particularly in children. Functional stereotactic surgery has also been used in the past and more recently deep brain stimulation has shown efficacy in a case of Holmes’ tremor caused by a thalamic abscess.9 Pharmacological treatment of Holmes’ tremor with levodopa or dopamine agonists may be beneficial, but results are disappointing in non-vascular aetiologies.7 We felt that, given the longstanding nature of the lesion and the minimal impact on the patient’s quality of life, watchful waiting was the appropriate management plan in this case.
Learning points
-
A rare but important cause of isolated Holmes’ tremor is thalamic tumour.
-
This is most likely due to disruption of cerebello–thalamo–cortical pathways.
-
Management may be watchful waiting, open or endoscopic surgical resection, radiotherapy or radiosurgery, depending on aetiology and degree of symptoms.
Acknowledgments
Professor Andrew Lozano, Consultant in Neurosurgery, Western Hospital, Toronto, Canada with whom the patient was reviewed in clinic.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.