Article Text

Statistics from Altmetric.com
Description
Giant cell arteritis (GCA) is a vasculitis involving branches of the external carotid artery, but also large vessels.1 We present the case of a panaortitis leading to the diagnosis of GCA.
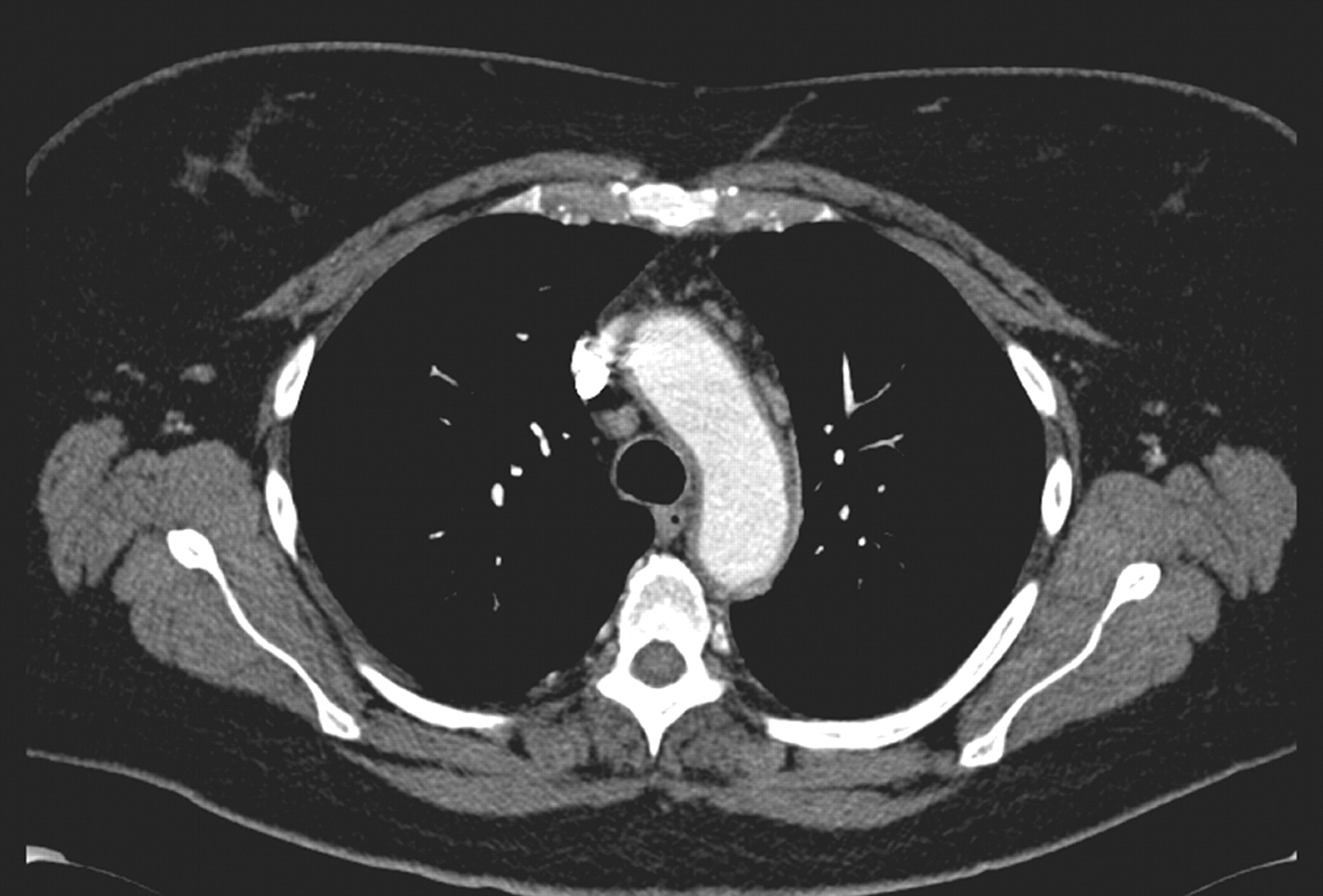
A 54-year-old woman, a smoker with an otherwise unremarkable medical history, was admitted for fever of unknown origin for 3 months duration, associated with asthenia, weight loss and vesperal perspiration. She did not take any medications. Physical examination was normal. Biological tests were only remarkable for high values of fibrinogen and protein C-reactive and inflammatory anaemia. A search for anti-neutrophil cytoplasmic antibodies was negative. Thoracoabdominal computed tomography (CT) scan revealed an aortitis of the whole aorta (fig 1). Transthoracic echocardiography was normal. Duplex ultrasonography of cervical and upper limb arteries revealed an aneurysmal aspect of the left axillary artery. Right temporal arterial biopsy yielded a typical histological diagnosis of GCA, although the patient never exhibited any cranial signs of GCA. Following treatment with steroids, the fever and asthenia rapidly disappeared, with normalisation of biological parameters and regression of the aortitis.

{kind=link}
Contrast enhanced computed tomography scan showing a regular circumferential thickening of the aortic wall at the arch level (arrows).
Thickening of the thoracic aortic wall, if assessed by CT scan, is present in half of GCA patients,2 and large artery complications are reported in around 20%, including dissection, aneurysm and stenosis.3 Although an aneurysm of the axillary artery has never been reported in GCA to our knowledge, our case suggests that it may be related to the arteritis. Physicians must also be aware that cranial signs of the disease are often lacking when faced with large vessel involvement in GCA.2,3
Acknowledgments
We acknowledge the patient.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.