Article Text

Summary
This brief case presents a well patient in whom an electrocardiograph abnormality consistent with an accessory pathway was found during a routine procedure. We present the electrocardiographs, explain the underlying condition, and consider why the abnormality was revealed in this manner.
Statistics from Altmetric.com
Background
This useful teaching case reminds hospital physicians to be wary of even apparently incidental electrocardiograph abnormalities. The case prompts and provides revision of accessory pathway disorders and what should be done in an emergency. This condition is important to recognise because traditional treatments for common arrhythmias, such as digoxin and verapamil, can be dangerous or fatal.
Case presentation
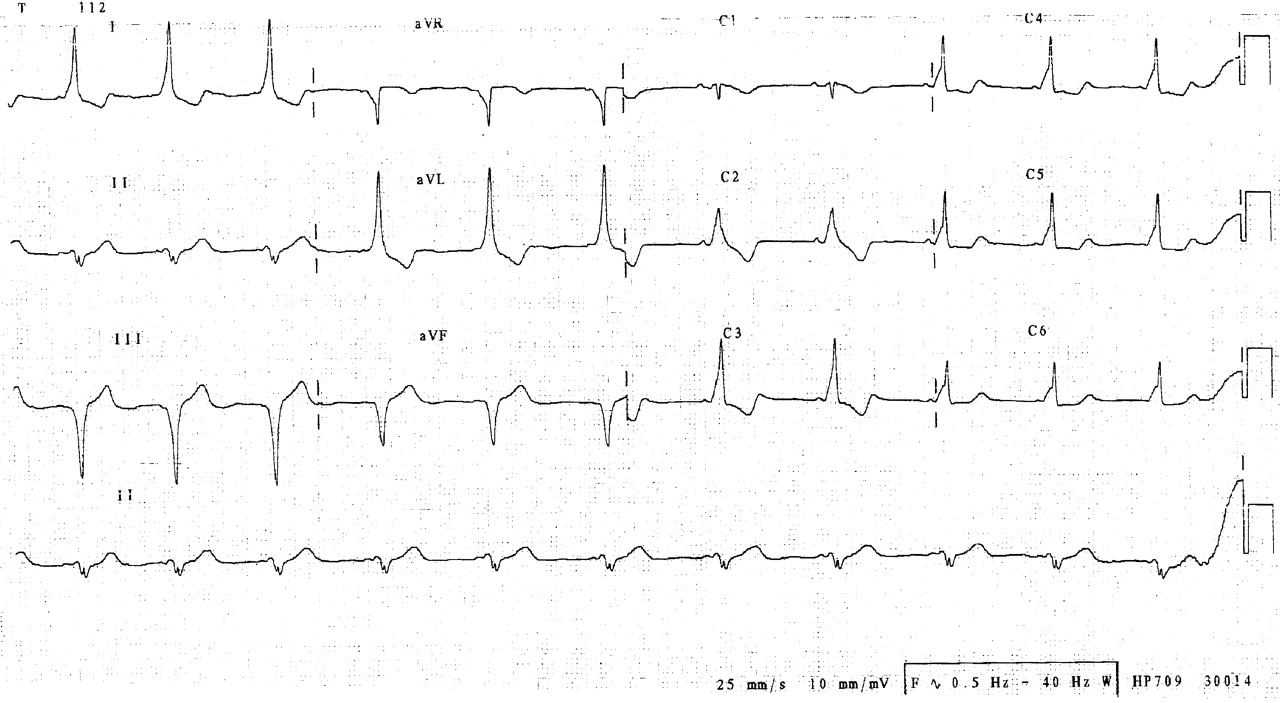
A 51-year-old woman underwent routine laparoscopy for the assessment of recurrent pelvic pain. She gave a history of palpitations 2 years ago, but a previous Holter monitor showed only sinus rhythm. There was no other past medical history of significance and no regular medication. The preoperative electrocardiogram (ECG) was normal. General anaesthesia was induced using propofol (200 mg IV) and fentanyl (100 μg IV) without muscle relaxant. Within 3 min of the laparoscopy starting, the morphology of the ECG was noted to change on the cardiac monitor (fig 1). No haemodynamic compromise occurred and laparoscopy continued uneventfully. A 12 lead ECG in recovery continued to show the abnormality (fig 2) but returned to normal within 10 min. The potassium value was 3.6 mmol/l, but all other electrolytes were normal. An echocardiogram showed normal sized and functioning ventricles. Outpatient Holter monitoring revealed several asymptomatic episodes of the abnormality but exercise testing was normal. The patient is undergoing regular follow-up under cardiology.

Rhythm strip showing the abnormality which developed during laparoscopy.

A 12 lead ECG showing the abnormality persisted shortly after the procedure.
Discussion
The ECG abnormality noted during laparoscopy is a shortened PR interval, broadening of the QRS together with a ‘slurred up-stroke’, or ‘delta wave’ (fig 3). These are features of ‘pre-excitation’ and occur when there is an accessory pathway within the heart. Here, we briefly discuss accessory pathways, and the dangers of arrhythmias occurring within this setting. We also consider why anaesthesia and surgery may reveal this abnormality.

{kind=link}
{kind=link}
{kind=link}
The abnormalities are marked on this figure to show the key electrocardiographic features of an accessory pathway, such as Wolff–Parkinson–White syndrome.
Wolff–Parkinson–White syndrome
Wolff–Parkinson–White (WPW) syndrome is the most common ‘pre-excitation’ syndrome, in which an abnormal accessory pathway connects the atria and ventricles, located in the atrioventricular sulcus.1 Sometimes called the bundle of Kent, this pathway allows atrial electrical activity to circumvent the His-Purkinje system, conducting in an antegrade, retrograde or bidirectional manner. This allows part of the ventricle to become excited before it should and manifests on the ECG as a shortened PR interval, slurring of the QRS upstroke (delta wave) and increased duration of the QRS complex and an atypical QRS complex axis. The incidence of this ECG pattern in the general population is 0.1–0.3%.2
In concealed WPW, the resting ECG is normal without pre-excitation. In some cases this is because conduction through the accessory pathway is intermittent. This pattern is more benign with a lower risk of death though patients may have unexplained paroxysmal supraventricular tachycardias (SVT).3–5 Occasionally, the accessory pathway activates the ventricle at the same time as conduction from the atrioventricular node (AVN), meaning pre-excitation is absent and the ECG appears normal.3–5
Arrhythmias in WPW
SVTs and atrial fibrillation (AF) can occur in WPW. They may be triggered by atrial, junctional or ventricular premature beats. The conducting properties of the accessory pathway can allow circus movement of electrical impulses between the atria and ventricle. Depending on the conducting properties, the arrhythmia can be a narrow or broad complex tachycardia, with or without evidence of pre-excitation. If a broad complex tachycardia occurs it should be urgently treated as ventricular tachycardia.
AF in WPW can occur in up to a third of patients and can be lethal.1 The accessory pathway has a shorter refractory period than the AVN and can allow rapid conduction of atrial electrical activity to the ventricle.1 In AF, a broad complex and irregular tachycardia at rates >250 beats/min may occur. This can rapidly degenerate into ventricular fibrillation (VF).
All arrhythmias in young patients with ‘normal hearts’ could represent a WPW related arrhythmia and should be treated with extreme caution. Traditional treatments of AF such as adenosine, calcium channel blockers, β-blockers and digoxin all prolong the AVN refractory period and therefore increase accessory pathway conduction. This could lead to VF requiring immediate defibrillation. Therefore, emergency synchronised DC cardioversion should be the treatment modality of choice, and should be performed immediately.
Patients with WPW should have 24 h Holter monitoring and echocardiography. Stress exercise testing may help. Patients with a confirmed SVT caused by an accessory pathway should undergo electrophysiology testing for risk stratification and radiofrequency ablation in symptomatic patients. Some patients may have drug treatment with flecainide.
Effects of general anaesthesia on the conducting system
Patients with known WPW are more likely to have tachyarrhythmia during anaesthesia.6 Anaesthesia can reveal concealed or intermittent pre-excitation in those with normal ECGs.7 Inhalational agents, including halothane, isoflurane and enflurane, slow conduction in both the normal conducting system and accessory pathways.8 Therefore, these agents are less likely to expose a hidden accessory pathway and trigger an SVT during anaesthesia.8
In this patient a combination of propofol and fentanyl was used. Human studies have shown that fentanyl alone does not affect conduction in the accessory pathway in WPW.9 However, in dogs fentanyl does prolong AVN conduction and therefore promote conduction via the accessory pathway, and it is known to enhance cardiac vagal tone.10
Studies using propofol have shown no effect on the sinoatrial node, intra-atrial conduction, and the refractory periods of the AV node and accessory pathway. Therefore, propofol is commonly use during electrophysiological studies of accessory pathways.11 In one reported case, however, propofol causes pre-excitation to disappear.12
However, adding fentanyl to a propofol infusion appears to enhance cardiac vagal tone and alter sinus node function.10 It has been shown that enhanced vagal tone slows normal conduction by increasing AVN refractoriness but does not affect accessory pathways.13 Therefore, enhanced vagal tone promotes accessory pathway conduction and pre-excitation.13 In the presence of enhanced vagal tone a premature atrial ectopic could trigger an SVT.10 Provided haemodynamics remain stable and an arrhythmia does not occur, anaesthesia and the operative procedure can continue. Any arrhythmias will require prompt treatment with electrical cardioversion.
A wide variety of surgical procedures are associated with sudden changes in heart rate and blood pressure. This is attributed to a vagal response and leads to bradycardia in the majority of patients. In those with an accessory pathway, this surgically enhanced vagal tone will promote accessory pathway conduction and also trigger an SVT. In the patient presented here, it is likely that pelvic laparoscopy further enhanced the vagal tone established by propofol and fentanyl anaesthesia to reveal a hidden accessory pathway.
Learning points
-
Accessory pathway disorders, such as Wolff–Parkinson–White syndrome (WPW), can be hidden and present incidentally. They should be referred to cardiology for investigation and follow-up.
-
Arrhythmias occurring in those with WPW should be treated with caution and preferably with DC cardioversion.
-
Anaesthetic agents have differing affects on the cardiac conducting system and should be chosen with care in those with an accessory pathway.
-
Surgery that is associated with vagal responses may trigger unstable tachyarrhythmias that require urgent DC cardioversion.
Acknowledgments
SSN had idea for submission, researched and wrote the manuscript. SWD edited the manuscript and is guarantor for final submission.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.