Article Text

Statistics from Altmetric.com
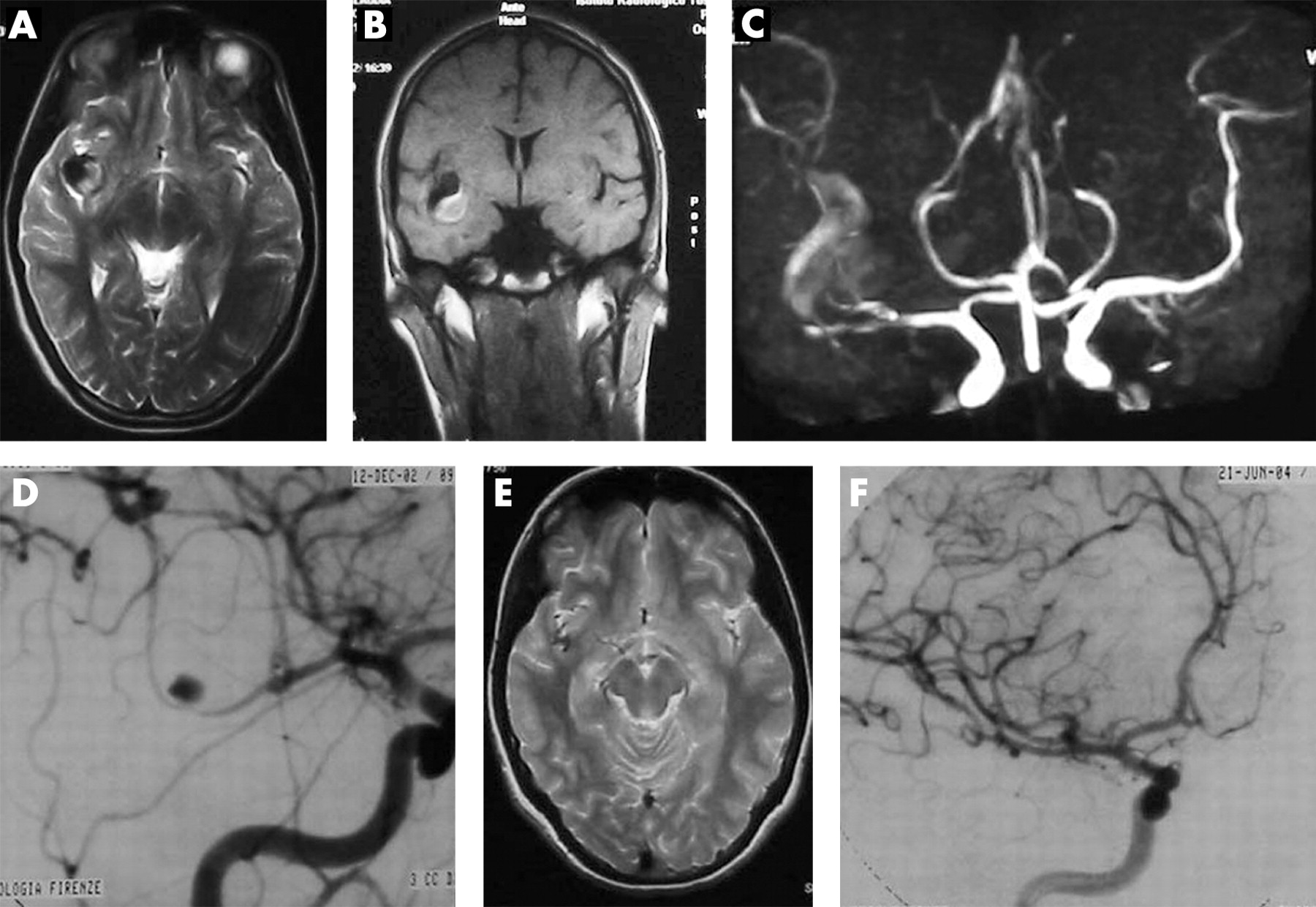
A 16-year-old female was admitted to hospital due to intermittent right-sided headaches. On admission, physical and neurological examinations yielded no unusual findings. She underwent a MRI and angiography (MRI-MRA) (fig 1A–C) that showed a fusiform dilatation of the right middle cerebral artery (MCA) division branches. A subsequent plain CT scan of the head and a lumbar puncture revealed no subarachnoid bleeding. Two weeks later, catheter angiography (DSA) showed a stenosis-dilatation-stenosis pattern (pearl-and-string sign) of the lower division branch of the right MCA, consistent with dissection (fig 1D). To exclude a mycotic or infective cause, the patient was analysed with a complete cardiological check-up that yielded no positive findings. The girl was discharged as she was completely asymptomatic. A follow-up MRI (fig 1E) and DSA (fig 1F) 18 months later showed complete resolution of the initial findings. Giant (>2.5 cm in length) fusiform aneurysms are spindle-like lesions that involve the main part of the arterial circumference. They account for 5–17% of giant aneurysms, which, in turn, represent 3–13% of all intracranial aneurysms.1 Their location at the division (M2–M3) branches of the MCA is fairly uncommon, although they may occur—particularly in young people. These aneurysms may be associated with trauma, infection, inflammation, atherosclerosis or spontaneous dissection. Giant fusiform aneurysms are usually a cause of cerebral ischaemia or subarachnoid haemorrhage. Their natural history is not known, but partial thrombosis is common; however, complete spontaneous resolution is very rare and often associated with ischaemic symptoms.2 Most unusually in our patient, complete resolution of the lesion occurred without clinical events. In the past, two cases of aneurysms with asymptomatic total resorption have been reported.2 3 Crescent-like high signal intensity around a signal void is the hallmark of dissection on MRI. The high signal corresponds to an intramural haematoma. However, the rate of intramural haematoma shown on MRI ranges from 32% to 100%, according to the timing of MRI. DSA still remains the “gold standard” imaging method for diagnosis, MRI-MRA being an alternative when repeated examinations are required.4 The double lumen sign (intimal flap with contrast stagnation), stenosis with dilatation (pearl-and-string sign), dilatation without stenosis (string sign) and stenosis without dilatation or occlusion (tapered occlusion) represent the hallmarks of arterial dissection on DSA. Stenosis is usually not focal but extensive, and serial changes are seen on follow-up examinations. Management of intracranial giant fusiform aneurysms is controversial; surgical and endovascular approaches (eg, proximal occlusion or trapping with or without bypass) are both technically demanding and high-risk procedures.5 The spontaneous regression of the lesion without clinical consequences in our patient suggest that conservative treatment may represent a valid alternative in patients with asymptomatic giant fusiform dissecting cerebral aneurysms.

{kind=link}
Acknowledgments
This article has been adapted from Cellerini M, Mangiafico S. Asymptomatic spontaneous resolution of a giant fusiform M2–M3 dissecting aneurysm in a teenager Journal of Neurology, Neurosurgery and Psychiatry 2008;79:863
Footnotes
Competing interests: None declared.
Patient consent: Informed patient consent was obtained for publication of the case details described in this report.