Article Text

Statistics from Altmetric.com
An elderly man presented with recurrent episodes of abdominal pain associated with pronounced distension and vomiting. Plain abdominal x ray demonstrated loops of distended small bowel with collapse of the colon. A contrast computed tomography (CT) scan of the abdomen was performed which revealed a mass in the region of the terminal ileum with concentric lines of wall enhancement, suggesting intussusception (fig 1). The obstructive symptoms settled. Colonoscopy, performed to elucidate the nature of the mass, confirmed intussusception of the terminal ileum into the caecum/ascending colon (fig 2). No mucosal or submucosal masses could be identified. Symptoms of small bowel obstruction recurred and a laparotomy was performed.


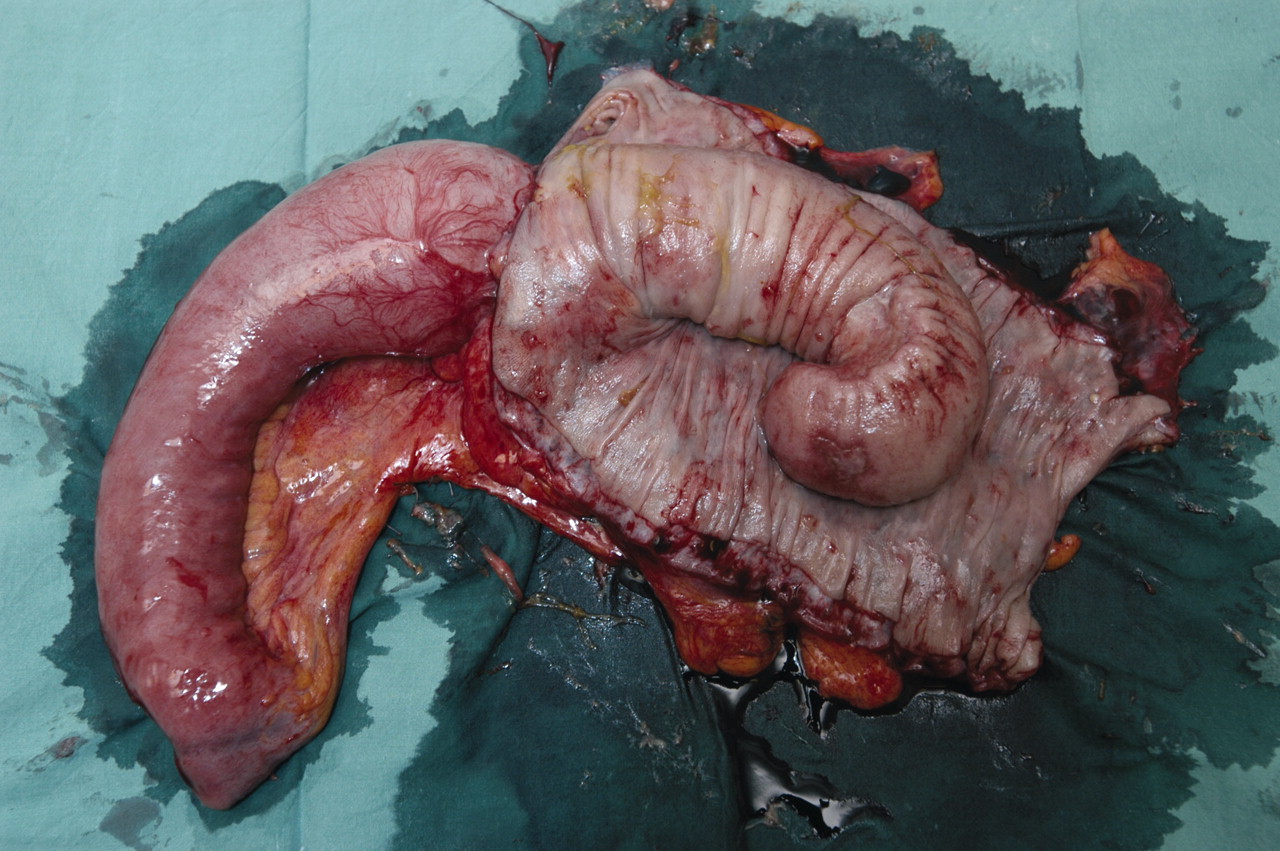
At operation the small bowel was obstructed by the intussusception of the terminal ileum into the right colon. A right hemicolectomy was performed. The post-resection specimen confirmed a 15 cm ileocolonic intussusception with no masses within the ileum (fig 3). Histology demonstrated ischaemic necrosis secondary to intussusception with no evidence of malignancy.
{kind=link}
{kind=link}
{kind=link}
Intussusception describes the telescoping of one segment of the gastrointestinal tract into an adjacent segment. It is relatively uncommon in adults, accounting for only 5% of all cases of intussusception.1 In approximately 90% of cases an identifiable lesion is found to be acting as a lead point, of which up to 65% may be malignant.2,3 Symptoms are often non-specific, including abdominal pain and vomiting, which are only seen in about 20% of patients with an acute presentation. This frequently leads to a delay in diagnosis, particularly in cases of subacute or chronic intussusception.
Ultrasound and CT findings are characterised by the finding of a “target-like” mass, with central dense echoes and eccentric lines of sonolucency. At endoscopy an obstructing lesion or underlying mass acting as a lead point may be identified. Biopsy is not generally recommended in chronic cases due to the potential risk of perforation where ischaemia or necrosis has occurred.
The treatment of adult intussusception remains controversial. In general primary bowel resection is performed with preliminary reduction only attempted if the small bowel is involved, the bowel segment is thought to be viable, or if no malignancy is suspected.
Footnotes
Competing interests: none.