Article Text

Statistics from Altmetric.com
Scleromyxoedema is an uncommon disease that is clinically characterised by widespread progressive induration of the skin of the fingers and extremities. Patients may also have cysts and urticarial lesions.1 Most patients with this disorder present with monoclonal paraproteinaemia, mainly IgG lambda. Oesophageal abnormalities with dysphagia, muscle weakness, dyspnoea with restrictive lung disease and cor pulmonale, pericardial effusions, central nervous system abnormalities and neuropathies, arthralgias and Raynaud’s phenomenon have been observed and may be associated with significant morbidity and mortality.2
Various agents have been proposed in case reports and small series for treatment of this condition with variable success. IVIG and thalidomide in combination may be an effective novel treatment of scleromyxoedema. Additionally, skin ultrasonography, a non-invasive test, may become a useful diagnostic and disease activity monitoring tool.3
The 40-year-old female patient presented with skin nodules in legs and hardening of skin especially in the forearms (figs 1–4). This is not typical for scleroderma and so we proceeded to skin biopsy, which revealed deposition of mucinous material in the dermis. In scleroderma, there is excess collagen fibre deposition. The patient has no dyspnoea or dysphagia. Protein electrophoresis was normal.

The left forearm showing variable-sized nodules related to the extensor surface.

Another nodule related to anterior surface of the leg.

The two hands show variable-sized nodules, skin hardening and preserved finger creases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
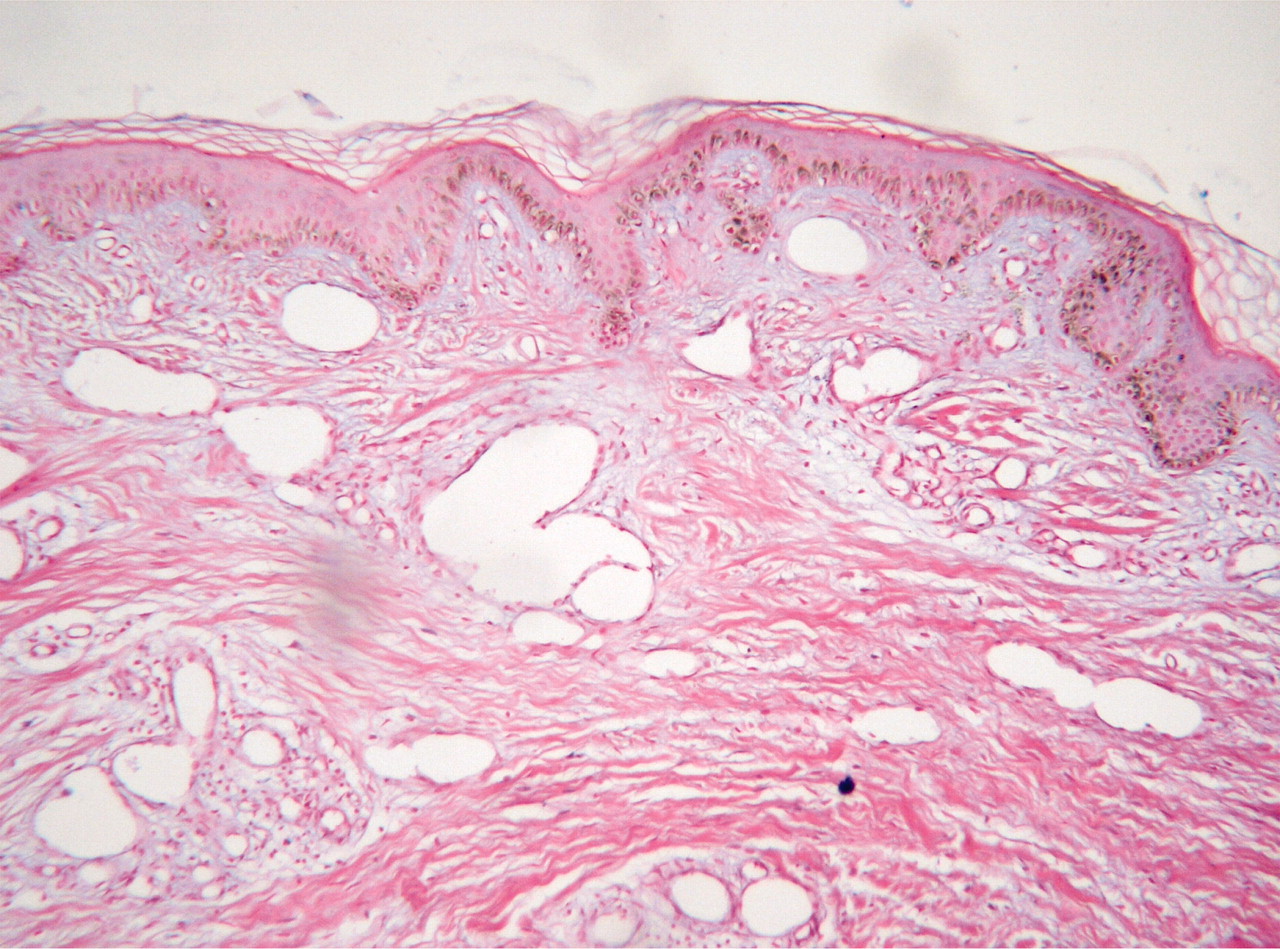
A skin biopsy from a nodule over the forearm with adjacent skin revealed deposition of mucinous material in the dermis stained by H&E.
LEARNING POINTS
-
Scleromyxoedema is a skin disease with or without systemic manifestations not related to scleroderma or to myxoedema (normal thyroid function).
-
The diagnosis of scleromyxoedema is a clinicopathological diagnosis.
-
Treatment is usually unsatisfactory and may include phototherapy, steroids and creams but results are poor.
Acknowledgments
Dr Mohamed El Daroty, Professor of Dermatology, who revised the skin biopsy.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.