Article Text

Statistics from Altmetric.com
Abrikossoff’s tumours, or granular cell tumours (GCTs), are uncommon, usually benign, neoplasms that are thought to derive from Schwann cells of the peripheral nerves. They can originate anywhere in the body but are most frequently found in the head and neck, particularly in the oral cavity. When they are located in the breast, physical examination, mammographic, ultrasonographic findings and pathologic examination may suggest breast malignancy. Immunohistochemical analysis is required for definitive diagnosis. GCT is negative for oestrogen receptor, progesterone receptor and queratin and strongly inmunoreactive to S-100 protein. Core needle biopsy preoperatively is able to establish the definite diagnosis and help to avoid surgical overtreatment. The surgical treatment of choice is wide local excision.
We report a case of metachronous GCT of the breast and tongue in a 42-year-old woman who presented with a palpable mass in the upper inner quadrant of the left breast.
A 42-year-old woman presented with a palpable mass in the upper inner quadrant of the left breast. Four years before, a GCT of the tongue was excised.
Physical examination revealed a 3×4 cm firm mass without skin alteration or nipple discharge.
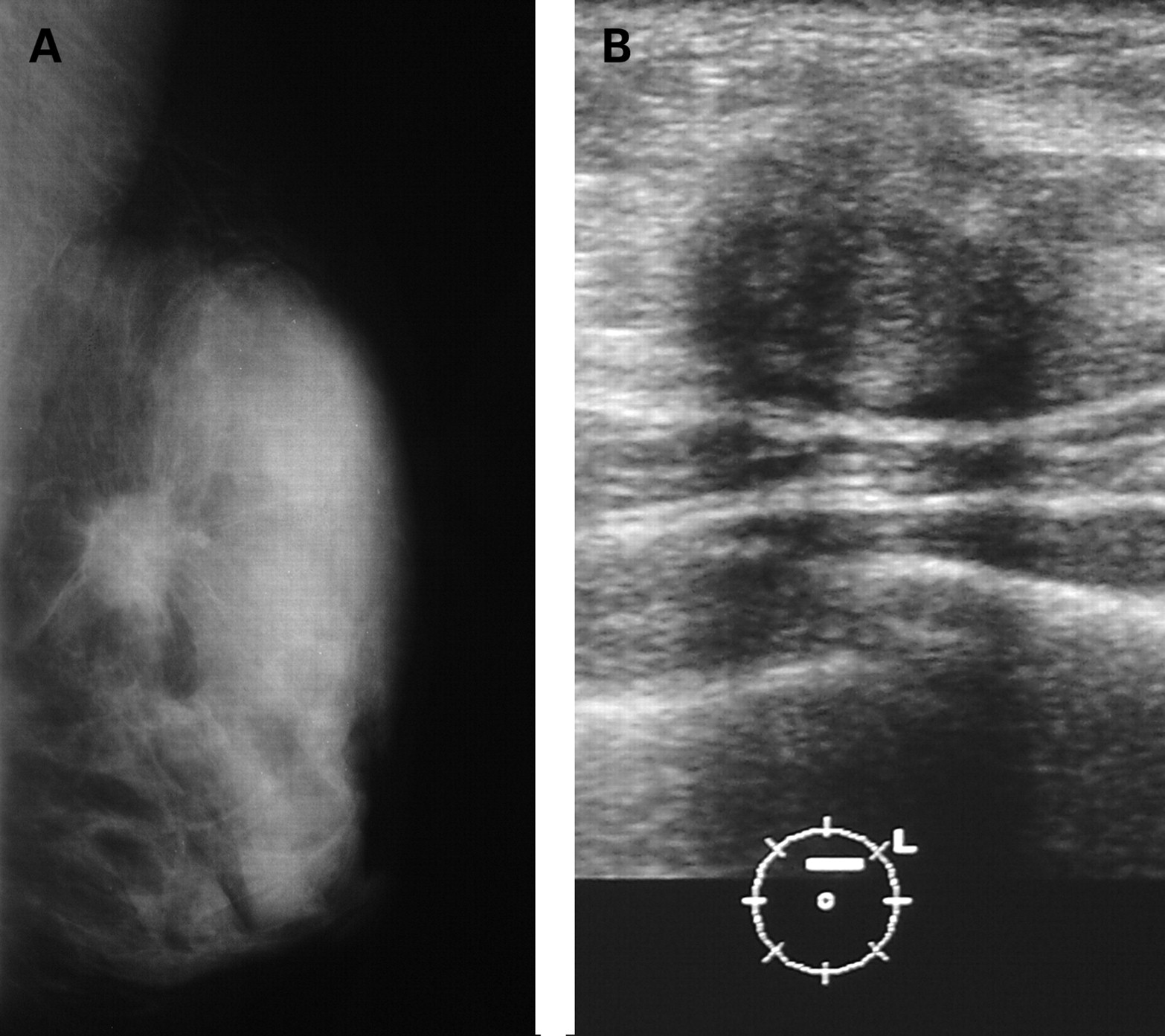
Mammogram showed a high density, spiculated mass without calcifications (fig 1A).

(B) Ultrasonography: well circumscribed, hypoechoic mass with posterior shadowing.
Ultrasound revealed a 3 cm diameter hypoechoic, well circumscribed mass with posterior acoustic shadowing (fig 1B). The core needle biopsy result was positive for GCT (Abrikossoff’s tumour). A tumorectomy was performed and the postoperative pathologic examination confirmed the diagnosis of granular cell tumour (fig 2), identical to the previous tongue neoplasm.

{kind=link}
{kind=link}
GCT was first described by Abrikosoff in 1926 as granular cell myoblastoma,1 but recent investigations favour a neural origin derived from Schwann cells.2–4 It is rare and usually presents as a benign solitary lesion, but multifocal and malignant forms are known to occur. Microscopically, GCT comprise sheets and cords of polygonal cells with round small nuclei and abundant eosinophilic granular cytoplasm. GCT is negative for oestrogen receptor, progesterone receptor and queratin and strongly inmunoreactive to S-100 protein, that established its neural origin. So, this justifies its frequent location in the upper inner quadrant, parallel to the skin distribution of the supraclavicular nerve. It is a relatively uncommon lesion, which most often affects the tongue (30%), skin or subcutaneous tissue, although it may occur at any body site. Six per cent of GCTs affect the breast, mainly of pre-menopausal women.
Due to the infiltrative growth pattern of CGT, it is frequently confused clinically and mammographically with breast carcinoma. A firm, fixed mass with overlying skin changes can be seen. At mammography it is often a small, spiculated mass without microcalcifications. Ultrasound may show a hypoechoic mass with posterior shadowing. Preoperative tissue diagnosis is mandatory to avoid unnecessary radical mastectomy because GCT is usually benign and is cured with wide local excision.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication