Article Text

Summary
A previously well 13-month-old child presented to our institution with a pneumonia which developed into a tension pneumatocoele. Management was conservative and the patient fully recovered. Streptococcus pneumoniae type 7F was isolated and is not covered by the current heptavalent vaccine.
Statistics from Altmetric.com
BACKGROUND
It is unusual for a streptococcus pneumonia to develop into a pneumatocoele, and extremely rare for this to be a tension pneumatocoele.
There is also a potential public health issue that needs to raised regarding the new Prevenar vaccine.
CASE PRESENTATION
The 13-month-old first male child of Caucasian, non-consanguineous parents became unwell with high fevers, poor eating and drinking. He was previously fit and well, fully vaccinated and there was no significant family history. He developed a rash and was seen at the local hospital. There he tolerated fluids and was discharged the same day. Over the next 9 days he continued to spike temperatures in the evening and have reduced intake and fewer nappies. He then had 3 days of noisy breathing and cough, with one day of diarrhoea, at which point he presented to a different district general hospital. His radiograph on admission showed left sided consolidation and effusion, that was later confirmed by ultrasound. He was commenced on intravenous cefuroxime and flucloxacillin. The blood culture grew a fully sensitive pneumococcus, but as he continued to be pyrexial he was commenced on clarithromycin. He was later changed to intravenous amoxicillin clavulanate (Augmentin) and clarithromycin. A week after admission he had a repeated ultrasound, which demonstrated a multiseptated effusion at the left upper zone anteriorly (1.5×4×5cm), with extensive consolidation of the lung. It was therefore arranged that he be transferred to the local tertiary centre.
INVESTIGATIONS
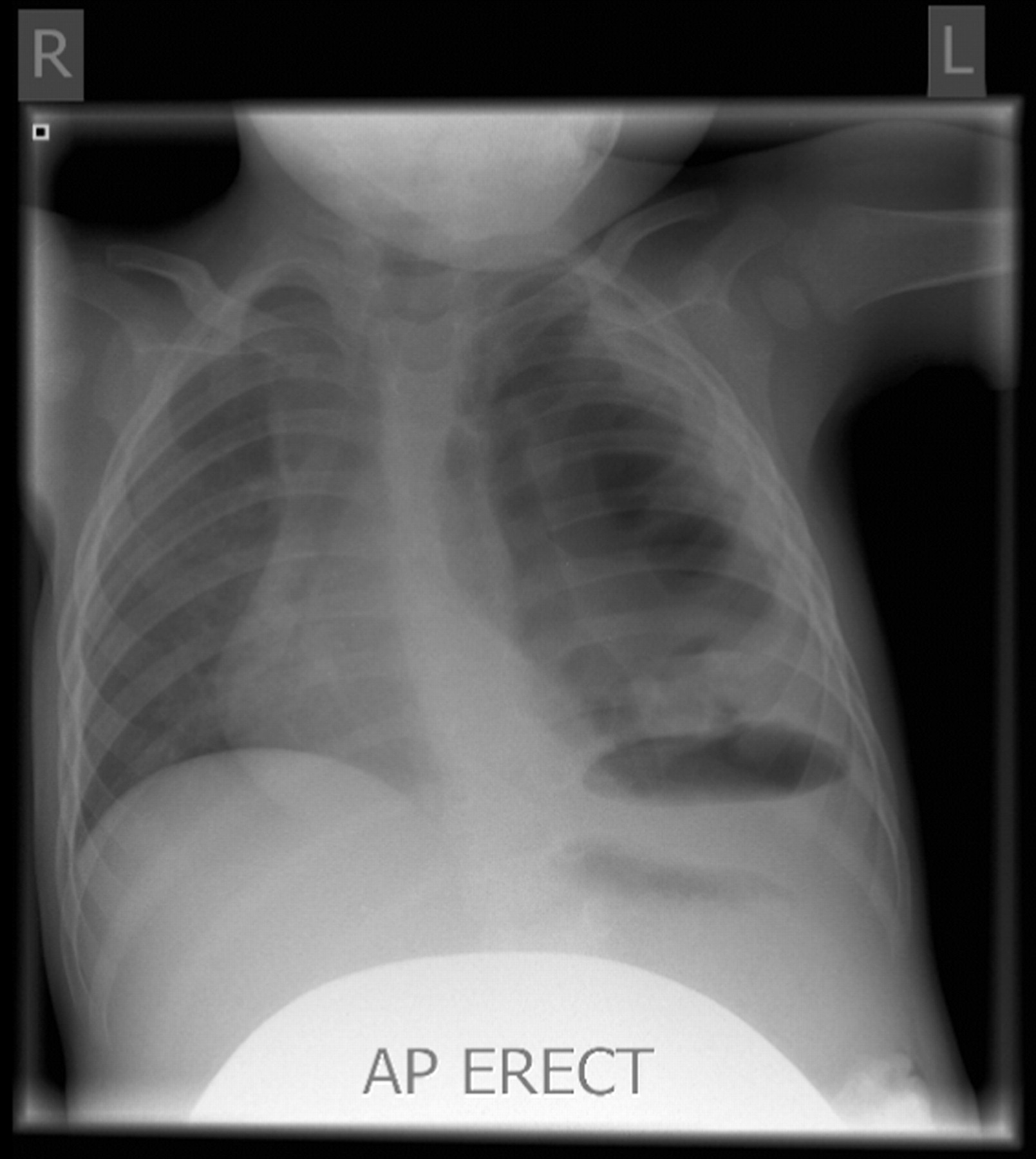
Within 24 h of arrival, a repeat ultrasound was “consistent with a complex pleural collection, such as an empyema”. A further chest radiograph the next day demonstrated mediastinal shift to the right, appearing to be under tension (fig 1). The patient appeared lively and active, with the parents reporting that he was “the best he had been in ages.” A computed tomographic (CT) scan done on the same day (fig 2) showed “Large communicating cysts within the left pleural cavity. Some left perihilar consolidated lung with air bronchograms leading into small cysts. Larger cyst is more peripheral, but does communicate with an air bronchogram. All cysts probably intrapulmonary. There is a fluid level in the basal cysts.” It was decided these were pneumatocoeles.

Chest radiograph showing a tension pneumatocoele.

{kind=link}
{kind=link}
Computed tomography scan showing pneumatocoeles.
OUTCOME AND FOLLOW-UP
The patient was treated conservatively with a further 3 days of intravenous antibiotics followed by a prolonged course of oral amoxicillin and clindamycin. A chest x ray undertaken a week after the CT scan showed some improvement, with less mediastinal shift and improving consolidation. He had a declining C reactive protein (CRP) concentration. Clinically he was felt to be improving with better air entry on the left side and trachea less deviated. He was discharged and is being followed up as an outpatient. His most recent radiograph, taken 3 months since discharge, has been reported as normal.
DISCUSSION
Although pneumatocoeles are felt to be rare complications, one study in Sao Paulo reported an incidence of 8.3% out of 394 pneumonias over 2 years, with spontaneous involution in 28 (85%). Pleural fluid culture was negative in 51% cases; in positive cultures, Streptococcus pneumoniae was the most common agent.1 A recent retrospective case notes review from Boston also reported that the most common organism was S pneumoniae, but that the incidence of other organisms was increasing.2 This study reported that the outcome in these children was good, with all of those that had follow-up having normal pulmonary function tests and complete normalisation of lung parenchyma on CT after a few months of hospitalisation.2
LEARNING POINTS
-
The incidence of complications associated with pneumococcal pneumonia, including necrotising pneumonia, parapneumonic effusion, thoracic empyema, and lung abscess has increased dramatically in UK children over the past decade,3 and the reason for this is not known.
-
The Prevenar vaccine was introduced into the UK childhood vaccination schedule in 2006. After the vaccine’s introduction into the US vaccination programme in 2000, the incidence of pneumococcal parapneumonic empyema has continued to increase in US children, because of a non-significant increase in serotype 1 disease and the emergence of disease related to other serotypes not covered by the vaccine.4
-
The serotype in this case was 7F. The serotypes of S pneumoniae included in the Prevenar vaccine are 4, 6B, 9V, 14, 18C, 19F, and 23F. Thus this serotype was not covered by the vaccine. This raises the question of whether vaccination could be causing serotypic drift, resulting in more severe infections as the general population becomes exposed to unseen serotypes of S pneumoniae?
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication