Article Text

Statistics from Altmetric.com
A 77-year-old man, with a history of Staphylococcus aureus thoraic aortic aneurysm (TAA) with graft replacement 4 years ago, presented with chest pain and massive haematemesis. A pale appearance with air hunger and hypotension (72/42 mm Hg) and were noted. Endotracheal intubation, intravenous fluid and blood transfusion were performed. Laboratory analysis revealed a white blood cell count of 42 900 cells/mm3 with 93.5% neutrophils, haemoglobin 9.1 g/dl and creatinine 2.4 mg/dl. Chest x ray (fig 1) and CT angiography (CTA) of aorta (fig 2) disclosed an aortoesophageal fistula (AEF). Emergency surgical repair was suggested, but the family did not consent to the procedure. The patient died the next day. Blood cultures grew Staphylococcus aureus 1 week later.

Chest x ray revealed a widening mediastinum with enlargement of aortic arch and tortuosity of descending thoracic aorta (long black arrow) and distended stomach in upper abdomen (short black arrow).
{kind=link}
{kind=link}
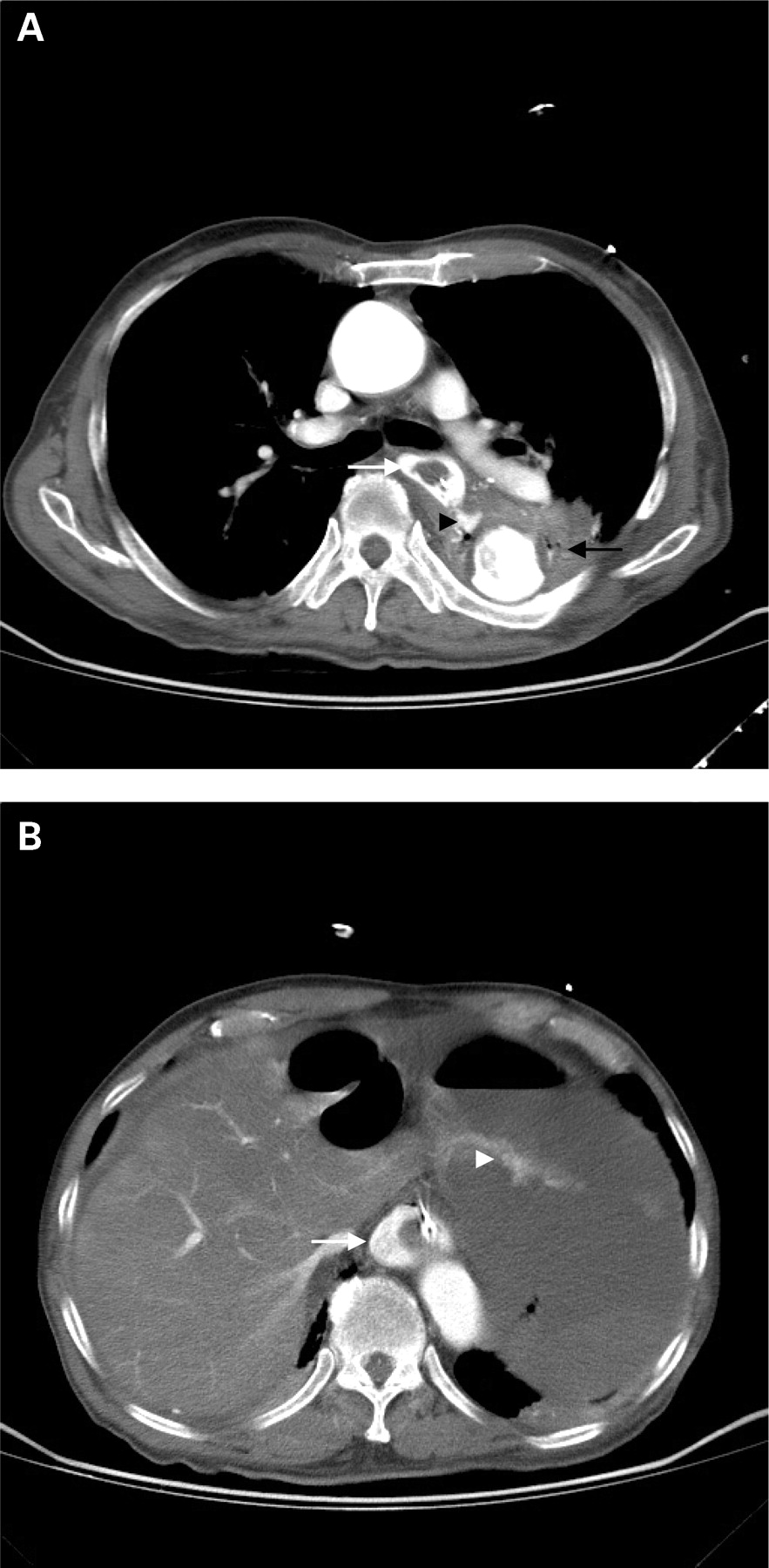
CT angiography of aorta demonstrated a graft thoracic aorta with air bubbles inside the thrombus and surrounding tissues (black arrow in A), and contrast media extravasation (black arrow head in A) between thoracic aorta and oesophagus and coating oesophageal mucosa (white arrow in A and B) from the level of descending thoracic aorta into the stomach (white arrow head in B), which disclosed an aortoesophageal fistula.
The incidence of mycotic aneurysms is estimated to be about 0.65% to 1.3% of all aortic aneurysms. The predominant micro-organism associated with mycotic aneurysms is Staphylococcus aureus.1 The incidence of AEF is approximately 0.01% to 0.08% of massive upper gastrointestinal bleeding (UGIB).1,2 TAA is the most common aetiology of primary AEF and the Chiari triad of AEF is midthoracic pain or dysphagia, a sentinel episode of haematemesis and fatal exsanguinations.3 In a patient who is haemodynamically unstable with UGIB of an unknown aetiology, who has a history of repair for aortic dissection/aneurysm, evidence of a tortuous aorta or aneurysm by chest x ray or who exhibits the Chiari triad, the presence of AEF should be entertained.3 CTA of the aorta delineates secondary signs suggestive of AEF, such as oesophageal compression or air bubbles inside the aneurysmal thrombus and surrounding tissues.2 Prompt surgical repair or an endovascular stent/graft replacement is recommended as soon as possible.1–3
LEARNING POINTS
-
Aortoesophageal fistula (AEF), most commonly associated with thoracic aortic aneurysm (TAA), is a rare complication and an uncommon cause of massive gastrointestinal (GI) tract bleeding
-
CT angiography (CTA) of the aorta is a mandatory survey for AEF.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.