Article Text

Statistics from Altmetric.com
A 56-year-old woman with type 1 diabetes presented with a 2 day history of vomiting and was diagnosed with diabetic ketoacidosis. Following initial improvement on therapy she developed abdominal distension and was referred to the surgical team for further evaluation. Clinical examination revealed obvious small bowel obstruction (fig 1A). Computed tomography (CT) demonstrated a hernia passing through the right obturator foramen (fig 2) causing the small bowel obstruction.
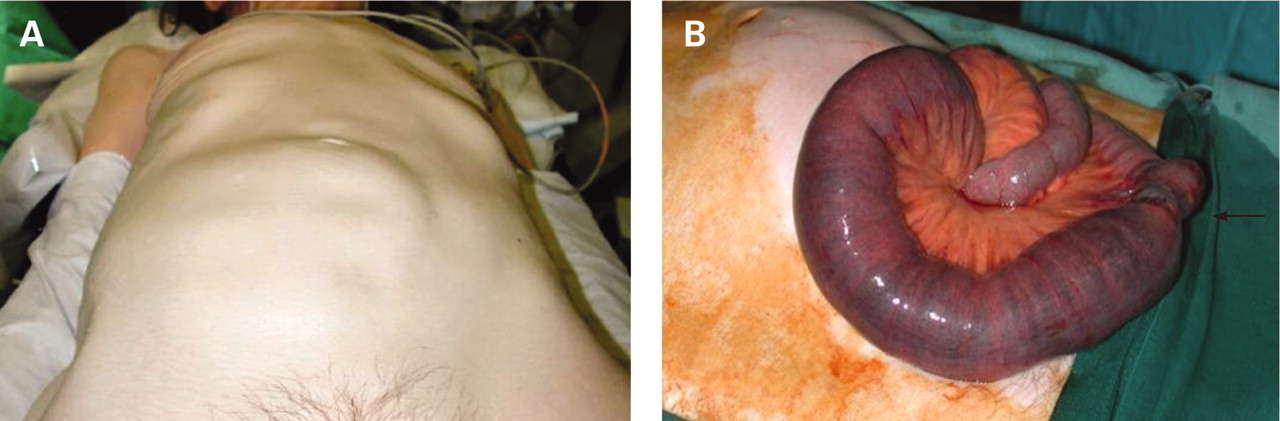
Image of abdomen demonstrating clinically obvious dilated loops of small bowel (A) and associated surgical findings of Richter’s type hernia, distended loops, necrotic portion (arrow) and collapsed distal small bowel (B).

{kind=link}
{kind=link}
Abdominal CT demonstrating hernia which has passed through the obturator foramen lying behind the right pectineus muscle.
An obstructed right obturator hernia of Richter’s type was confirmed at laparotomy (fig 1B). Limited small bowel resection with closure of the obturator defect was undertaken and the patient made an uneventful recovery.
In the absence of specific symptoms and signs, there is often difficulty in diagnosing obturator hernias, resulting in delayed diagnosis and poor outcomes.1 The obturator hernia is a rare and potentially the most lethal of all abdominal wall hernias.2 It typically occurs in elderly women with a history of weight loss with associated reduction of fat in the obturator canal. The patient commonly presents with non-specific obstructive symptoms. A swelling may be felt clinically in Scarpa’s triangle, however it is often overlooked as it is covered by the pectineus muscle. Howship-Romberg sign (pain down the anteromedial thigh on movement) is rarely seen. The diagnostic modality of choice is CT3 which can, as in our case, demonstrate a hernia or mass with associated small bowel obstruction. Obturator hernias may be treated successfully with an open or laparoscopic technique with suture or synthetic mesh closure.
Acknowledgments
South Infirmary - Victoria University Hospital, Cork, Ireland
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.