Article Text

Statistics from Altmetric.com
Description
Solitary extramedullary plasmacytoma is often seen in patients with long-standing multiple myeloma, but can rarely be a presenting feature of initial disease.1–4 The most common presenting symptom is proptosis seen in almost 81% followed by ptosis, diplopia, periorbital oedema and ecchymosis.4 A 37-year-old man was referred to our clinic with right-sided severe axial proptosis, conjunctival chemosis, total ophthalmoplegia, exposure keratopathy without any light perception. He had a previous history of biopsy-proven multiple myeloma in anterior mediastinum and left testes for which he had received chemotherapy and radiotherapy 2 years back. He had presented to the ophthalmologist with a history of gradually increasing right-sided ptosis associated with eyelid swelling, diplopia, headache of 1 week duration. Radiological imaging showed presence of right-sided intraconal lesion of size 3.6 cm × 1.0 cm with invasion of medial rectus muscle. Incision biopsy was advised, however, the patient went into systemic inflammatory response syndrome and had multiple intensive care unit admissions, and was was lost to follow-up. Within a span of 2 months, his proptosis had been rapidly progressing and while he reached us, he had severe proptosis with central retinal artery occlusion and no light perception. Contrast-enhanced CT scan showed ill-defined enhancing intraconal mass measuring 1.73 cm × 8.3 cm (TR × AP) involving the whole orbit extending till the cavernous sinus. The differential diagnoses at this point were orbital plasmacytoma, lymphoma and non-specific orbital inflammation. In view of non-salvageable globe with no light perception and rapidly increasing proptosis with intracranial involvement, eyelid sparing orbital exenteration was done and the mass was confirmed as plasmablastic variant of plasmacytoma immunopositive for CD38 and MUM-1 but were lambda restricted (figure 1A–C). The patient underwent radiotherapy for 16 cycles, chemotherapy with bendamustine (in view of better brain penetration), thalidomide and dexamethasone. At 6 months follow-up, his socket was healthy without any recurrence, yet, he doesn’t prefer to wear an orbital prosthesis and continues to be under our constant supervision (figure 1D).

{kind=link}
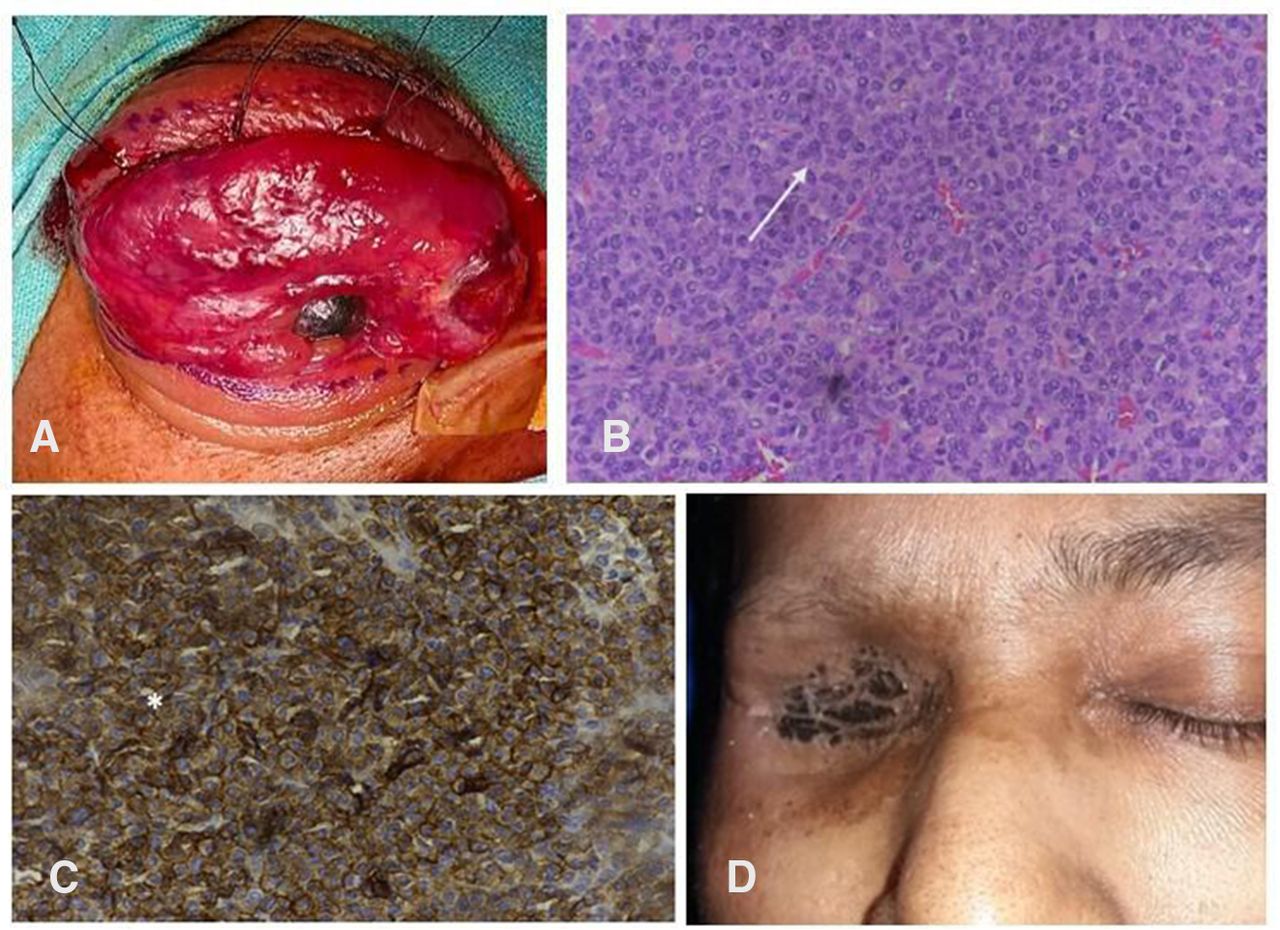
(A) Clinical photo showing right-sided massive proptosis and exposure keratopathy planned for eyelid-sparing orbital exenteration with traction sutures in the upper eyelid. (B) H&E stain 40 × histopathology photo showing sheets of plasma cells with intranuclear inclusions. (C) Immunohistochemistry staining showing cells immunopositive for CD38. (D) Postexenterated healthy socket after subsequent radiation therapy.
Previous literature review regarding orbital involvement in multiple myeloma reveals that it can mimic orbital cellulitis, orbital abscess, dacryoadenitis, lacrimal gland tumour, eyelid solitary nodule and metastases.5–9 However, out of 220 published case reports and series regarding orbital involvement in multiple myeloma, mostly including case reports and small case series, only few case reports have established coexisting orbital tumours such as T cell lymphoma, squamous cell carcinoma, amyloidosis and, very rarely, aspergilloma (other than plasmacytoma) in patients with prior history of multiple myeloma.9–12 Few authors advocate radiation therapy without waiting for the histopathology confirmation and it has shown good restoration of vision and most importantly globe salvage.13 14
We have the opinion that patients with a history of biopsy-proven extramedullary plasmacytomas in the recent past and presenting with orbital involvement palliative radiation therapy can be started early while awaiting histopathology. This could effectively prevent rapid disease progression and may increase the chances of preserving the globe. The availability of a frozen section can serve as an useful adjunct in making an initial diagnosis. Due to the immunocompromised status of these patients, there are chances of acquiring lung infection and systemic inflammatory response syndrome and resulting multiple intensive care unit admissions, as in our patient, due to which the histopathology got delayed and globe salvage could not be done. Survival rates in patients with extramedullary plasmacytomas are already low regardless of the tissue involved.15 16 Therefore, they need early palliative radiation therapy to prevent disease progression which is usually very rapid and can lead to irreversible vision loss as has happened in our patient.
Learning points
Orbital plasmacytoma can be a relapsing feature in patients with multiple myeloma.
Although histopathological analysis is essential in the diagnosis, management and prognostication of relapse in multiple myeloma, palliative radiotherapy can be initiated in patients with rapid progression, bilateral presentation and in patients unfit to undergo biopsy procedures due to unstable systemic condition.
It is possible to salvage the globe and vision if radiation can be started early during the relapse.
Ethics statements
Patient consent for publication
Footnotes
Contributors BP contributed to the original concept and was the primary surgeon. AK and BM provided data and contributed to the analysis. PM provided histopathological data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.