Article Text

Statistics from Altmetric.com
Description
We hereby present a case of a woman in her 60s with bilateral iridoschisis and advanced glaucomatous optic neuropathy. Her visual acuity and intraocular pressures were 20/200 and no perception of light and 14 and 28 mm Hg in the right and left eye, respectively. The right eye had early nuclear sclerosis with a cup–disc ratio of 0.7–0.8:1 and asymmetric neuro-retinal rim (figure 1A,C), while the left eye had hypermature cataract and optic-nerve head cupping on B-scan ultrasound (figure 1B,D). Swept source anterior segment optical coherence tomography demonstrated anterior bowing of iris with split between the anterior and posterior iris stroma confirming the diagnosis (figure 2A,B). Glasses were prescribed to rehabilitate the right eye and it was explained to the patient that she would have no sight in the left eye. They were counselled to follow-up regularly.
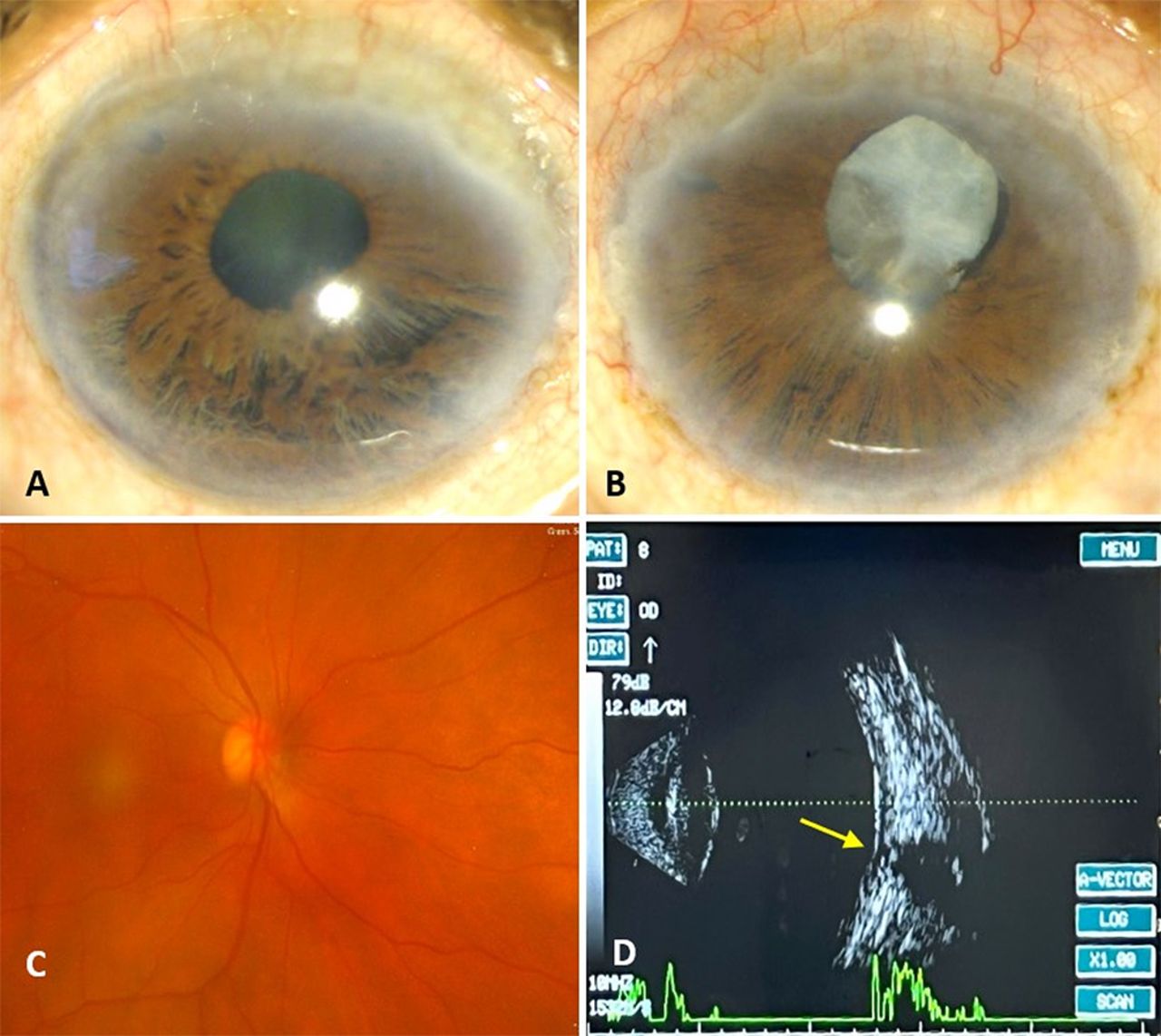
Slit-lamp images of right (A) and left (B) eye with thick arcus senilis, superior pannus, ‘shredded’ appearance of inferior iris. Right eye has early nuclear sclerosis while left eye had hypermature cataract. Fundus of right eye (C) highlights a 0.7–0.8 cup–disc ratio and ultrasound B-scan of left eye (D) shows optic nerve head cupping (arrow) with otherwise anechoic posterior segment.

{kind=link}
{kind=link}
Anterior segment optical coherence tomography of right (A) and left (B) eye showing bilateral disorganised anterior iris stroma with an intact posterior iris layer. There is evident associated narrowing of anterior chamber angle with relative pupillary block in the right eye.
Iridoschisis is a multifactorial rare ocular morbidity which is defined as separation of anterior iris stroma from posterior stroma and muscle layer. It was earlier assumed to be genetic (mostly autosomal dominant); however, most studies reported it to occur sporadically. It may also be age-related or secondary to trauma, glaucoma, or syphilis. It usually presents bilaterally in the 6th to 7th decade and involves the inferior iris. It is known to be associated with glaucoma, interstitial keratitis, keratoconus, lens subluxation, and corneal decompensation. The common embryological origin of posterior corneal layers and iris stroma through neural crest cells may suggest an inter-related pathogenesis between iridoschisis and corneal manifestations.1 Glaucoma is associated in two-third cases with primary angle closure. Other forms like chronic open-angle or angle recession glaucoma have also been reported. Differential diagnosis includes irido-corneal endothelial syndrome and Axenfeld–Rieger syndrome. Timely diagnosis and management are vital to preserve vision in the ocular disorder.2
Learning points
Iridoschisis is a rare ocular entity which is diagnosed clinically. Imaging helps to confirm the diagnosis and study angle anatomy in these cases.
It is most commonly associated with glaucoma, keratoconus, corneal decompensation, interstitial keratitis, and lens subluxation.
Early diagnosis and regular follow ups may aid in timely management of associated glaucoma and other complications.
Ethics statements
Patient consent for publication
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: AB, TT, MT, TA. The following authors gave final approval of the manuscript: AB, TT, MT, TA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.