Article Text

Abstract
A fit and well young man presented to our emergency department in the UK. On examination, he had an isolated left-sided ptosis; he had a 3-day history of frontal headache which was worse on head movement. He lacked any clinical signs of cranial, orbital, or preseptal infection, and his eye movements were normal. Ten days before presentation, he tested positive for SARS-CoV-2. Inflammatory markers were moderately raised, and CT of the head did not reveal any vascular abnormality or intracranial lesion. Imaging revealed opacification, predominantly in the left facial sinuses, keeping with sinusitis. He was discharged the same evening with oral antibiotics and made a full recovery over the next few days. He remained well at 6-month follow-up. The authors convey their findings to raise awareness of a rare complication of sinusitis and to demonstrate the utility of CT imaging for diagnosing sinusitis and ruling out severe pathology.
- Emergency medicine
- Ear, nose and throat
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Acute sinusitis is a common upper respiratory tract issue with a yearly incidence of 1%–5% in the European adult population.1 The term ‘acute’ refers to complete resolution within 4 weeks from symptom onset. Sinusitis is caused by inflammation of the paranasal sinus mucous membranes and most cases are viral in origin. Adult presentation is commonly characterised by purulent nasal discharge, nasal congestion, facial pain and reduction in the sense of smell.2 We are reporting this rare presentation of a common health problem to raise awareness of this potential diagnosis when faced with a patient with isolated ptosis, after more serious pathologies have been ruled out. Moreover, referral to an ear, nose and throat (ENT) specialist should be kept in mind, especially on suspicion of an obstructing meatal lesion as the cause of sinusitis or in complicated disease. Notwithstanding, very few case reports convey a similar presentation of acute sinusitis in an adult; to the best of our knowledge, this case is particularly distinctive due to the recent COVID-19 infection and the lack of nasal discharge. Herein this report, we convey the case of a man in his 20s who had recently recovered from COVID-19, presenting with acute sinusitis in an extremely atypical fashion.
Case presentation
Patient information
A usually fit and healthy man in his mid-20s, with no prior history of sinus or ENT issues, presented to our emergency department in the spring of last year. He recovered from COVID-19 10 days before presentation; these symptoms lasted a week and consisted of a mild cough and generalised headache. Three days before presentation, he noted his left eye remained closed after waking up, and he concurrently noticed a pungent odour. Both symptoms worsened throughout the course of the day. Towards the evening, he developed a bilateral frontal headache, which was intensified by head movement. His headache worsened daily, eventually prompting him to visit the emergency department. He denied any vomiting, photophobia, neurological symptoms and trauma. He also had no visual or auditory changes. There was no prior surgical history, no known allergies, and he was not taking any regular medication.
Clinical findings
On inspection, he was fully alert and orientated and had a partial left-sided ptosis.
He was apyrexic, and his other vital signs were all within normal parameters. Ophthalmic examination demonstrated equal and reactive pupils, no periorbital swelling or discharge and normal fundoscopic findings. ENT examination revealed no nasal deformity, haematoma or discharge, and his ears and throat were normal. Neurologically, he was otherwise unremarkable.
Investigations
Full blood count showed mildly elevated white cell count (10.7×109/ L, normal range 3.7–9.5×109/L) and neutrophils (8.1×109/ L, normal range 1.8–7.5×109/L).
Serum biochemistry tests demonstrated a raised C reactive protein (61 mg/L, normal range<4 mg/L) and normal renal and liver function tests.
PCR testing was negative for SARS-CoV-2.
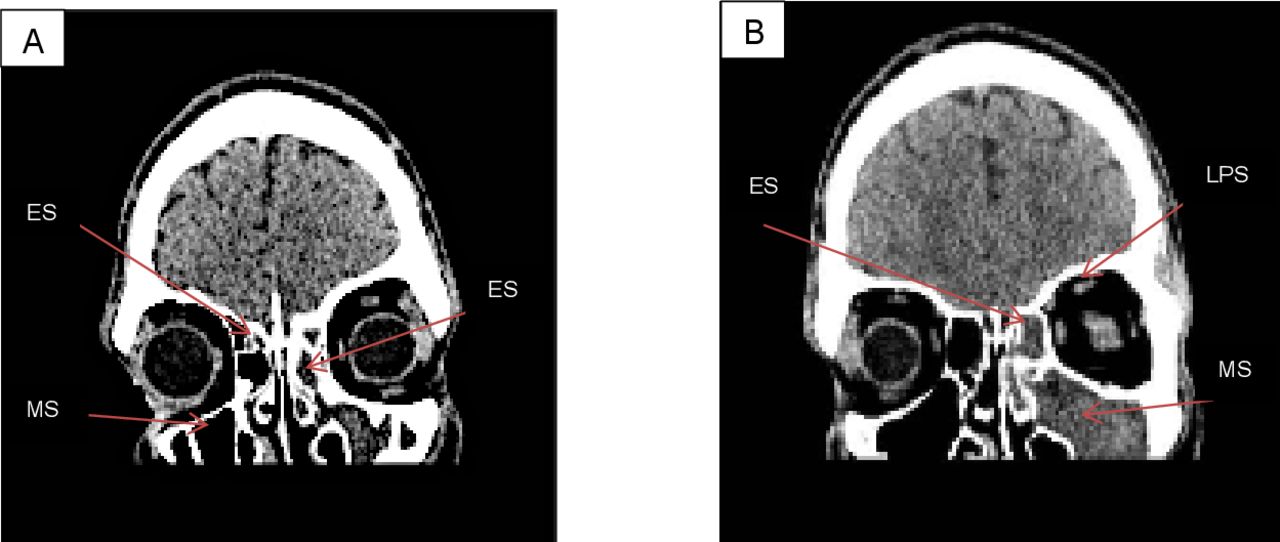
He underwent a non-contrast CT of the head to rule out any intracranial abnormality. CT imaging could not demonstrate any infarction, haemorrhage, aneurysm or mass lesion. However, there was complete opacification of the maxillary sinus (figure 1), frontal sinus (figure 2) and ethmoid air cells on the left side (figures 1 and 2). There was also minor partial opacification of the ethmoid air cells and frontal sinus on the right side (figures 1 and 2).
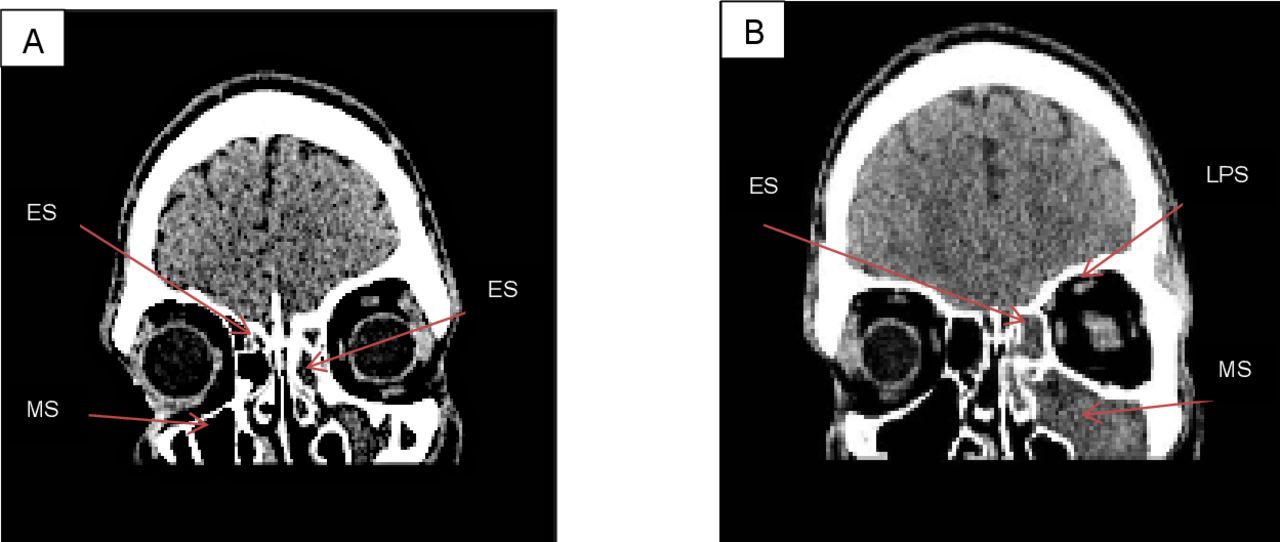
Both sagittal slice images display opacification of predominantly the ethmoid sinus (ES) and maxillary sinus (MS) on the left side. (A) No opacification of the right maxillary sinus but some opacification of the right ethmoid sinus. The location of the left levator palpebrae superioris (LPS) is arrowed in (B); this muscle is responsible for raising the upper eyelid.

(A,B) An axial slice view of opacification in the left-sided ethmoid sinus (ES) and frontal sinus (FS), respectively. (C,D) Marked left-sided frontal sinus opacification in the sagittal and coronal planes, respectively. There was no sphenoid sinus (SS) involvement at all on either side.
Imaging did not demonstrate any evidence of levator palpebrae superioris (LPS) injury, nor was there evidence of inflammation within the orbit.
Differential diagnoses
The raised inflammatory markers created suspicion of some underlying inflammatory process, although this may have been bacterial or post-COVID-19 related. PCR testing ruled out present COVID-19 infection.
The most concerning differential for us to rule out was an intracranial bleed, mainly due to the exertional relationship with the headache. The combination of ptosis and headache was very perturbing at the time; this is seen in posterior communicating artery aneurysms, whereby most symptomatic aneurysms cause oculomotor nerve palsy due to mass effect or through aneurysmal rupture.3 Moreover, a midbrain infarction or mass lesion, which could also cause a third nerve palsy, had to also be ruled out. There was no trauma or anticoagulation therapy, and because of the patient’s age, a cerebrovascular accident would have been very unlikely. The pupillary examination was essential as a patient presenting with mydriasis, without response to light, could harbour a compressive lesion.
Another differential for sudden onset unilateral ptosis—cavernous sinus thrombosis—can also be a complication of sinusitis; however, the ensuing pressure elevations in the cavernous sinus after 3 days would have likely caused other ocular signs as well as the involvement of the contralateral eye,4 both of which were absent in our patient.
The rapid nature of CT scanning meant that all these concerning diagnoses could be ruled out promptly.
Horner’s syndrome could not have occurred due to a lack of pupil constriction or anhidrosis. He was non-diabetic, making medical neuropathy unlikely to be the cause. Myasthenia gravis was kept lower in the differentials due to it commonly presenting with diplopia, and there was as a lack of fluctuating weakness of the LPS. Moreover, an orbital infection was deemed very unlikely due to no ophthalmoplegia or eyelid swelling. Figure 3 illustrates a flow chart of the differentials.

Differential diagnoses flow chart. Acute sinusitis was deemed the likely cause for the patient’s ptosis due to the left sinuses being mainly affected, other causes being ruled out, and a small number of case reports conveying similar findings in sinusitis. The authors speculate the mechanism being very localised inflammation, at the very distal aspect of the superior ramus of cranial nerve III (innervating the levator palpebrae superioris (LPS) muscle), with a possible association with the recent COVID-19 infection; see ‘Discussion’ for a description of a case report conveying influenza-like infection preceding transient, fully reversed ptosis, in five patients. CRP, C reactive protein. (Figure created by MOM—corresponding author.)
A very rare differential mentioned in case reports, with a very similar presentation, is myositis affecting only the LPS.5 6 However, given the rarity of such a diagnosis, this diagnosis was deemed extremely unlikely, and the CT did not show any evidence of LPS inflammation either.
Diagnosis
The official diagnosis was left-sided frontal, ethmoid and maxillary sinusitis, as well as right-sided ethmoid and frontal sinusitis; the aetiology was likely viral.
Outcome and follow-up
He was discharged with a 5-day course of oral co-amoxiclav. He completed his antibiotic course with no medication-related issues. Three days after discharge, his symptoms all cleared up; initially with his left-sided ptosis resolving, followed by his sense of smell returning to normal. He did not have any further sinus-related issues at 6-month follow-up, and he remained COVID-19 negative up till follow-up. On discharge, he was referred to ENT due to the complication which ensued. Moreover, although the paranasal sinus opacification was likely caused by inflammation, an obstructing lesion in the left middle meatus needed to be ruled out.
Discussion
Most sinusitis cases are not diagnostically challenging as the signs and symptoms, such as rhinorrhoea and congestion, are often characteristic, usually with a prior upper respiratory viral infection. Neurological or ophthalmological disease can seem more likely in the context of cerebral or ocular signs. Due to the proximity between the orbit and facial sinuses (figure 4), orbital complications secondary to sinusitis follow a logical trajectory. Infection and inflammation spreading to adjacent sites can result in the myriad of complications associated with sinusitis.
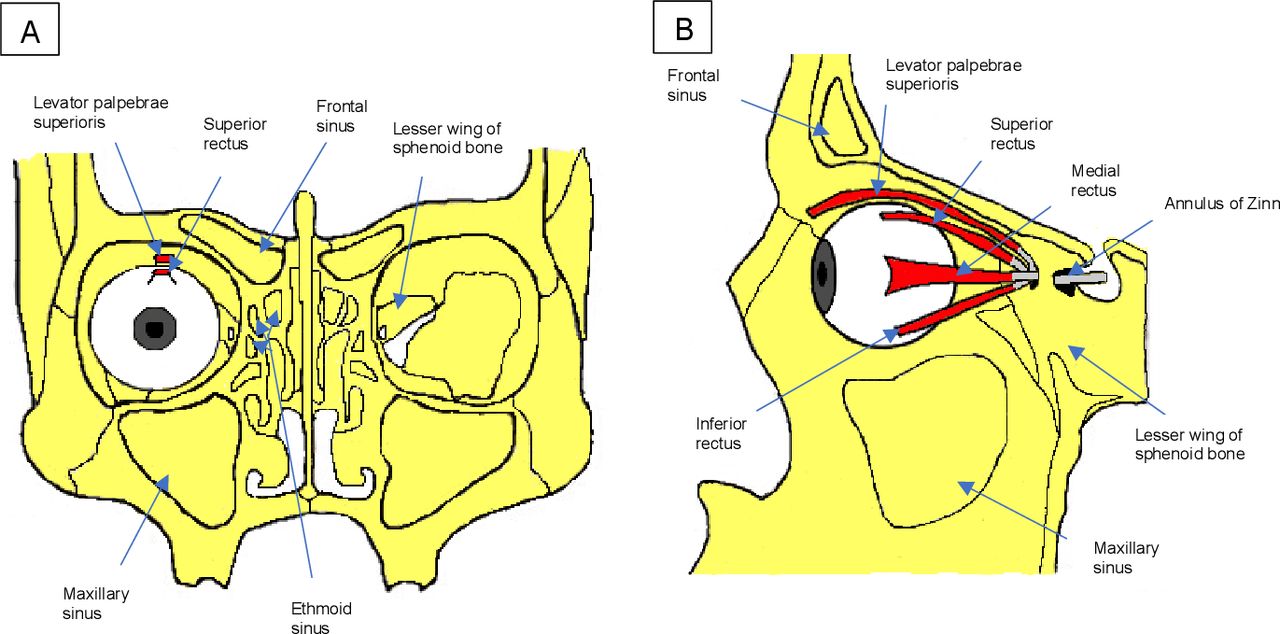
Anterior view of normal anatomy and relations of the sinuses to each other and the ocular muscles (A). Lateral left view (B). (A,B) illustrate the close proximity of the sinuses, in particular the frontal sinus, to the levator palpebrae superioris (and therefore the superior branch of cranial nerve III supplying this muscle), and thus convey how sinusitis, as in our case, can lead to complications, through adjacent inflammatory spread. (Figure created by MOM—corresponding author.)
Arising from the Annulus of Zinn, the LPS is the primary muscle that elevates and retracts the upper eyelid. This triangular-shaped muscle journeys above the superior rectus muscle, and its nervous innervation derives from the superior division of the oculomotor nerve.7 8 As such, damage to this muscle or its innervation can result in ptosis; myogenic, neurological or vascular abnormalities can result in this.9
The superior ramus of the oculomotor nerve penetrates the orbit via the superior orbital fissure. The authors speculate that due to very localised inflammation at the distal portion (figure 5), the LPS was compromised. Vertical eye movements were not compromised, thereby ruling out entire cranial nerve III (CNIII) involvement. However, Wilbanks et al10 conveyed this as a contentious mechanism when they were faced with a paediatric case of isolated ptosis due to pansinusitis. Their reasoning was that the inferior ramus is in very close proximity to the superior ramus; the inferior ramus innervates the inferior rectus, medial rectus and inferior oblique muscles, and also innervates the pupillary constrictors parasympathetically. The function of all these effectors was intact in both of our cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
We speculate the presenting ptosis to be due to inflammation over the superior ramus of the cranial nerve III (which innervates the levator palpebrae superioris (LPS) and the superior rectus muscles), distal to the branch innervating the superior rectus muscle; this would explain the full function of the superior rectus muscle. (Figure created by MOM—corresponding author.)
Arat et al11 described five cases of transient, fully resolving, isolated unilateral ptosis. All these patients had a preceding influenza-like illness; the authors speculated that the mechanism was a viral-induced injury to the terminal branch of CNIII or the LPS. It may be possible that our patient’s preceding COVID-19 infection could have played a similar role.
Other documented rare causes of isolated, unilateral ptosis have included myositis, orbital cellulitis10 and midbrain infarction.12
Despite very few cases in the literature mentioning isolated, unilateral ptosis caused by sinusitis, our case is distinct due to the lack of eye swelling and eye pain,13 nasal discharge13 14 and sphenoid sinus involvement.14 15 Moreover, our patient also had a recent novel viral infection, which could have contributed to the presentation.
We believe this report adds further awareness of how sinusitis can potentially present. Furthermore, the very recent COVID-19 infection, prior to the presentation, may have played a role in the pathophysiology underpinning his clinical manifestation, especially given the distorted sense of smell, which curiously manifested ten days after his last positive COVID-19 test.
Our case demonstrates the pivotal role of CT imaging in ruling out serious pathology and providing a rapid and subsequently benign diagnosis of sinusitis for the patient’s presenting symptoms. MRI would have been able to give a much more detailed view of the patient’s orbit, thus potentially addressing the conundrum regarding localised inflammation and mechanical causes for the LPS dysfunction.
National Institute of Clinical Excellence (NICE) guidelines recommend hospital admission for acute sinusitis, when there is presence of complication, namely, systemic infection, intracranial complications and orbital complications. However, ptosis is not explicity mentioned. ENT referral was made due to a complication arising and to ensure no sinister obstructive lesion was underpinning the presentation.
The raised CRP was indicative of a bacterial infection which, together with NICE guidelines recommending immediate antibiotics for sinusitis when complications arise, influenced the decision to discharge the patient with antibiotics. Sinusitis is often managed with nasal decongestants and steroid nasal sprays. However, nasal examination revealed no swelling, and the patient was not congested, so these were deemed unnecessary. It has been demonstrated that physician access to CRP results may decrease antibiotic prescribing for sinusitis, in the community setting.16
Conclusion
This report provides an addition to the case literature with regard to a rare cause of oculomotor nerve palsy. In addition, the authors’ speculation for a potential mechanism could provoke research into the pathophysiology behind such a presentation. Finally, clinically, this report will raise awareness regarding a potential complication of acute sinusitis to abet clinicians’ differentials when facing isolated, unilateral ptosis, particularly within the context of COVID-19 infection or another viral illness.
Patient’s perspective
I’ve never had sinus issues in the past, so this was all quite a shock. I’m relieved that my symptoms completely resolved, and I’ve been feeling healthy and myself since I recovered.
Learning points
The levator palpebrae superioris is responsible for elevating and retracting the upper eyelid and it is innervated by the superior ramus of cranial nerve III.
Ptosis is drooping of the upper eyelid, the aetiology of which can be a neurological, muscular or vascular abnormality.
Complete oculomotor nerve palsy involves ptosis, mydriasis (pupillary dilation) and diplopia (double vision).
Severe pathology responsible for ptosis, such as aneurysm, infarction or malignancy, can be both pupil-affecting and pupil-sparing.
CT imaging plays an excellent role in the acute setting to rule out intracranial abnormality as a cause for ptosis and can abet the diagnosis of sinusitis in atypical cases.
Ethics statements
Patient consent for publication
Footnotes
Contributors MOM was involved with collecting information for the case, writing the report, researching the literature and drawing the figures. AM and AO reviewed and edited drafts of the report. GM provided radiological expertise and offered guidance for the imaging components.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.