Article Text

Abstract
Macrocheilia, or lip enlargement, has a varied aetiology, but granulomatous conditions, both infective and non-infective, comprise a significant proportion of patients. Diagnosis starts with clinical investigations while histological examination is required for a definitive diagnosis. In the case presented, a young man presented with painless swelling of upper lip over the past 3 months. Given the clinical history and biopsy results, the diagnosis of granulomatous cheilitis was made which is considered a rare manifestation of metastatic Crohn’s disease. Treatment options remain debated, though in the situation presented a conservative approach was adopted, consisting of antibiotics and corticosteroid therapy, which resulted in significant remission in lip swelling without recurrence after a 3-month follow-up.
- Dermatology
- Inflammatory bowel disease
- Dentistry and oral medicine
Statistics from Altmetric.com
Background
Macrocheilia represents a great challenge in terms of diagnosis and therapeutic approach through the variability in morphological presentation and similarities to other dermatoses as from the incostant response to therapeutic options and the lack of a randomised control studies reported in the literature. Both systemic and local conditions can contribute to macrocheilia, which may even reveal a systemic disease. Granulomatous disease, as orofacial granulomatosis, is defined as a pattern of disease characterised by granulomatous inflammation with persistent and/or recurrent labial swelling, oral ulcers and a variety of other orofacial features, which is localised to orofacial region. The aetiopathogenesis of orofacial granulomatosis remains debate: it includes hypersensitivity to food or food additives or various dental materials, hereditary and genetic predisposition, inflammatory/immunological and microbiological factors, sarcoidosis, Crohn’s disease (CD) and Melkersson-Rosenthal syndrome.1 A detailed history and physical examination may help narrow the differential, but a biopsy of the lesion is often necessary for diagnosis. Handa et al presented a clinic-pathological study of 28 patients having chronic macrocheilia. Out of 28 patients, 13 patients (46.4%) had granulomatous cheilitis and diagnosis was made by histological examination. Miest et al presented a retrospective study of 76 patients complaining lip swelling which had biopsies performed, 40 (47%) had granulomatous inflammation.2 Granulomatous cheilitis is considered a rare manifestation of metastatic CD (MCD) which is known as a great mimicker and is often misdiagnosed.3 In this situation, diagnosis is confirmed by a colonoscopy usually showing gastrointestinal involvement. In the absence of bowel disease, it may be difficult to distinguish Crohn’s cheilitis from Melkersson-Rosenthal syndrome, cutaneous sarcoidosis, tuberculosis or other granulomatous disorder. Tuberculin skin test could also be done to exclude mimickers of MCD.
Case presentation
A late adolescence presented to his family physician with a pronounced swelling on his right upper lip over the past 3 months. He was otherwise healthy. During the assessment, he stated that the lesion was usually pale pink, but on occasion became bright red. On skin examination, a 2 cm, not well-demarcated pink-coloured oval nodule was observed on his cutaneous central upper lip; the neoformation presented a median skin fissure (figure 1). First of all, tuberculin skin was done to exclude mimickers of MCD. Then, due to the inconsistency of the pathological features, it was necessary to schedule an MRI, followed by a punch biopsy. MRI reported superior macrocheilia with orbicular muscle component identifiable, incorporated and thickened with oedematous manifestations of the bundles (figure 2); these findings were not typical of CD-related cheilitis. Histological examination with H&E stain showed well-formed granulomas surrounded by mixed chronic inflammatory infiltrate of lymphocytes, Langhans giant cells and plasma cells present throughout the dermis extending into the superficial fat. Focal spongiosis and exocytosis were also noted. Examination by polarisation and stains for fungi and mycobacteria (periodic acid–Schiff staining), acid and alcohol-fast bacilli testing, Grocott’s methenamine silver stain, were negative. Suspecting granulomatous cheilitis as a metastatic Crohn localisation, a colonoscopy was scheduled showing coarsening involvement of the mucosal pattern in the terminal ileum (figure 3). A biopsy from the terminal ileum was taken, confirming the same pattern of the previous one. Given the clinical history and biopsy results, the diagnosis was made. Considering the clinical situation, various treatment options were discussed with the patient which opted to treat just the cheilitis lesion. This conservative approach imposed a strict and scheduled follow-up cooperating with the gastroenterology equipment. Marked improvement of the lesion was observed at his 3-month follow-up appointment (figure 4).

Clinical appearance at the first visit.
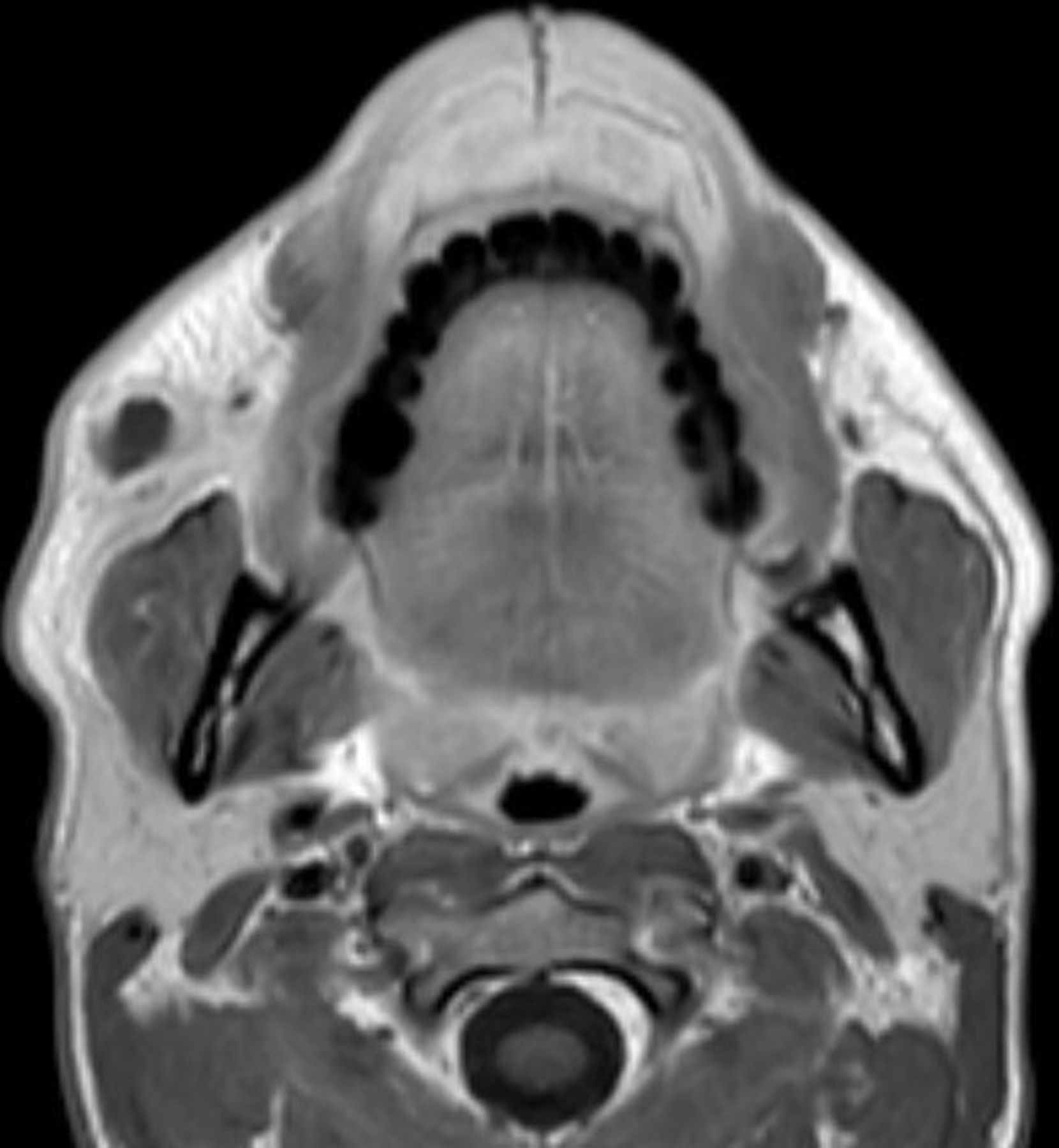
MRI.

Colonoscopy showing hyperaemic ileal mucosa with sores and erosions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Three months control.
Differential diagnosis
Macrocheilia is often misdiagnosed. Differential diagnosis is listed in table 1 including the whole granulomatous and non-granulomatous disease pattern.
Differential diagnosis of metastatic macrocheilia
Non-granulomatous disorders are mostly discriminate by the clinical examination. For example, hidradenitis suppurativa, impetigo, erysipelas present peculiar clinical features: erythematous boils, scabs in the context of an oedematous generally tender tissue. Orofacial granulomatosis is defined as recurrent or persistent facial soft tissue swelling in the absence of a specific previously diagnosed local or systemic disease. When it is associated with fissured tongue, lip swelling and facial palsy, the condition is more specifically associated as Melkersson-Rosenthal syndrome. On the other hand, isolated swelling or enlargement of the lip is known as granulomatous cheilitis which can be associated with sarcoidosis, CD (as a manifestation of MCD) and infectious diseases such as tuberculosis.4
Due the inconsistency of the pathological clinical features and considering the importance of a biopsy in same case, it is necessary to schedule an MR to characterise the lesion. MR narrows the diagnosis excluding, for example, vascular lesion and, moreover, allows to find out cleavage plan to programme an eventual surgery radical excision, especially if it could lead to nerve damage.5–7
In the case presented, biopsy results showed well-formed granulomas surrounded by mixed chronic inflammatory infiltrate of lymphocytes, Langhans giant cells and plasma cells present throughout the dermis extending into the superficial fat. Focal spongiosis and exocytosis were also noted. Histological examination gave the deep suspect of granulomatous cheilitis as a metastatic Crohn localisation supported also by examination by polarisation and stains for fungi and mycobacteria (periodic acid–Schiff staining, acid and alcohol-fast bacilli testing, Grocott’s methenamine silver stain, tissue cultures) which resulted negative.
Colonoscopy and a biopsy from the terminal ileum confirmed diagnosis.
Multispecialty coordination between primary care physicians and specialists such as maxillofacial, rheumatology, dermatology or gastroenterology will lead to faster and more efficient diagnosis and treatment.
Treatment
Although it has been reported that the cutaneous lesions of granulomatous cheilitis can spontaneously resolve, the vast majority are persistent. Unfortunately, there is no consensus on standard treatment as no clinical trials have been done to guide treatment.8 Several methods have been trialled varying in treatment length and response. Currently, the treatment is based on prednisone or prednisolone 20–40 mg daily or oral deltacortene 25 mg daily associated with antibiotics (metronidazole or doxycycline) if infection is present.9
In recalcitrant lesions originally treated with prednisolone, adding sulfasalazine 2–4 g/day systemically or sulfasalazine 3% ointment topically has been successful.9 Cyclosporine 4 mg/kg/day or 250 mg two times per day, azathioprine 2 mg/kg10 and 6-mercaptopurine have also shown some promise.
Severe refractory has been shown to respond to infliximab 400 mg infusions over a period of 7 weeks. In one case, methotrexate was also concurrently used with infliximab treatment.8 In patients who have had a prior infusion reaction to infliximab, certolizumab combined with methotrexate has recently been shown to resolve the cutaneous lesions. Recent studies indicated treatment with an anti-TNF agent (mainly ustekinumab) as the most recommended therapeutic option for granulomatous cheilitis (with or without CD) after failure of conventional treatments.11
Recurrence may take place with any of the above treatment modalities. Healed lesions can leave behind hypertrophic scars; however, these have been well treated with CO2 laser.9
In the case presented, considering the clinical situation, a conservative approach with doxycycline 100 mg and deltacortene 25 mg daily was chosen. This choice was supported by the patient but imposed a strict and scheduled follow-up cooperating with the gastroenterology equipment.
Outcome and follow-up
After the diagnosis of granulomatous cheilitis has been made, the patient was assessed also by gastroenterology equipment. Colonoscopy showed coarsening of the mucosal pattern in the terminal ileum even any kind of symptoms were not already present. A conservative approach with doxycycline 100 mg and deltacortene 25 mg daily was chosen. This choice was supported by the patient but imposed a strict and scheduled follow-up with periodic check every 6 months with a medical examination and evaluation of the global disease activity by blood chemistry tests (ESR, PCR, blood count, sideremia, liver and kidney function). A control colonoscopy was scheduled after a year or wherever necessary. Marked improvement of the lesion was observed at his 3-month follow-up appointment. The patient follow-up is still ongoing.
Discussion
Macrocheilia is a descriptive term commonly used to describe a variety of conditions that exhibit similar microscopic and clinical features. It usually describes persistent enlargement of the soft tissues of the oral and maxillofacial region especially upper and lower lips. Clinical presentation is very changeable but usually recurrent facial swelling, mainly in the lips with or without intraoral manifestations, is the single most common clinical feature at onset. The association with systemic conditions such as CD or sarcoidosis has been widely reported in literature. Moreover, it may precede CD by several years, frequently remaining the only evident active focus of the disease, and it may frequently represent an extraintestinal manifestation of CD in which oral lesions can be the first sign of an unknown intestinal disease.12 13
The detection of specific oral manifestations often preceded by painless gingival enlargement (diffuse lip and buccal mucosal swelling, oral cobblestoning, buccal sulcus ulceration and mucosal tags) and/or unspecific or ancillary ones (cheilitis, scaly perioral erythematous rashes and frank intraoral abscess formation, labial and tongue fissuring, glossitis and aphthous stomatitis) is mandatory for the early diagnosis of granulomatous cheilitis as a form of MCD.
Hence, the inflammatory bowel disease is a common illness that gastroenterologists encounter, about 40% of patients with CD have cutaneous symptoms, making the skin the most common site of extraintestinal involvement.14 This association between gut and skin can be classified into three broad groups described in table 2.
Classification of cutaneous manifestation of Crohn’s disease
No clear correlation between the development of MCD and severity of underlying Crohn’s has been established. In fact, the skin lesions may be present during, after and in rare cases before the presence of the inflammatory bowel disease. Cutaneous findings tend to occur more often with CD that involves the large bowel. Granulomatous cheilitis, such as other forms of oral CD, may precede, coincide with or follow the onset of gastrointestinal disease as in the case presented. In the absence of bowel disease, it may be difficult to distinguish granulomatous cheilitis from the Melkersson-Rosenthal syndrome.
Diagnosis of granulomatous cheilitis starts with clinical investigations but a biopsy of the lesion is always necessary.
As regards clinical examination, cutaneous manifestations of MCD have fairly variable morphology,3 for example, lesions present in intertriginous areas tend to have an ulcerated appearance; while lesions on the extremities tend to be erythematous and sometimes painful. Other morphological features include violaceous perifollicular papules and lichenoid papules found on the neck and lower limbs and erythematous plaques on the face and the extremities. In the situation presented, a 2 cm, not well-demarcated usually pink-coloured oval nodule was observed on his cutaneous central upper lip; the neoformation presented a median skin fissure. As mentioned, diagnosis is based on histological examination; microscopically, the dominant histological features of MCD are similar to the primary Crohn’s bowel lesions.3
MRI could be more useful than an ultrasound scan even in this case MRI findings were not typical of CD-related cheilitis.
Colonoscopy with a biopsy is always recommended: they will confirm diagnosis especially in the absence of clinical bowel manifestations as in this situation. In this situation, as in the most cases, biopsy confirmed the same pattern of the previous obtained from the lip.
Considering the clinical situation, various treatment options were discussed with the patient which opted to treat just the cheilitis lesion. This conservative approach imposed a strict and scheduled follow-up cooperating with the gastroenterology equipment. This choice was supported by the patient but imposed a strict and scheduled follow-up with periodic check every 6 months with a medical examination and evaluation of the disease activity by blood chemistry tests. A control colonoscopy was also scheduled after a year or wherever necessary. Patients with asymptomatic CD often develop complications during their clinical course because the absence of symptoms does not imply an absence of inflammation. The prognostic value and objectivity of endoscopy remains irreplaceable. Together with endoscopy, the role of less invasive techniques such as imaging tests (MR enterography, CT enterography and even echography, with and without contrast agent) and faecal markers (faecal calprotectin) has been reaffirmed in the literature in order to follow up the disease course. White blood cells, procalcitonin, PCR (C reactive protein), ESR (erythrocyte sedimentation rate), anti-TNF and its antibodies are precious indicators of inflammation. It is also mandatory to do periodic check of complete blood count, iron and ferritin, folate, transferrin, group B vitamins looking for anaemia. Finally is recommended to exclude faecal occult blood and a possible cancer degeneration.
Even treatment options remain underwhelming due to the lack of randomised control studies and varying responses of reported therapeutic methods, marked improvement of the lesion was observed after 3-month follow-up.
Patient’s perspective
‘I’m very happy about my situation now. I was very scared because I did not find any kind of help and the lesion on the face was growing up. A correct diagnostic and therapeutic approach gave me the opportunity to improve my health and prevent complications. I could choose from various treatment options and I opted for a conservative approach to treat just the cheilitis lesion which resulted very useful. After just 3 months, the upper lip lesion has improved. I am sure that gastroenterology equipment will manage in the best way any kind of systemic manifestation of my pathology.’
Learning points
Macrocheilia is a descriptive term commonly used to describe a variety of conditions that exhibit similar microscopic and clinical features.
Granulomatous cheilitis is a possible option in differential diagnoses of macrocheilia and is the rarest manifestation of metastatic Crohn’s disease.
Cutaneous findings may precede, develop concurrently with or follow gastrointestinal involvement.
A biopsy is always required for a definitive diagnosis.
A correct diagnosis and a well-targeted therapeutic approach led to an improvement of the clinical status.
Ethics statements
Patient consent for publication
Acknowledgments
None.
Footnotes
Contributors FF participated in acquiring patient data, performing surgery and in the patient follow-up, participated in photographs collection and in article composition. GG participated in article composition and correction. FC participated in article composition and correction. PG participated in article composition and correction.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.