Article Text

Statistics from Altmetric.com
Description
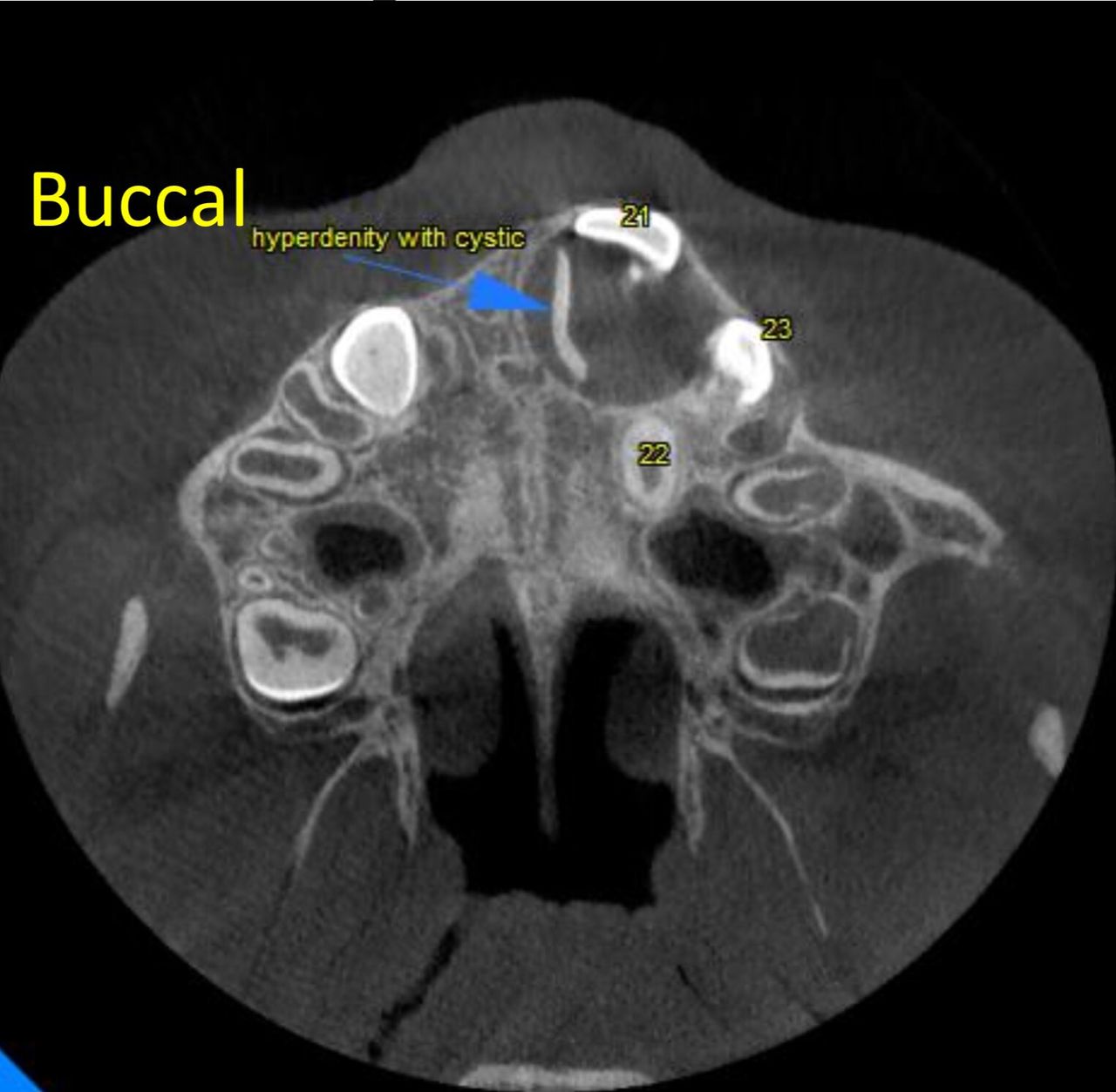
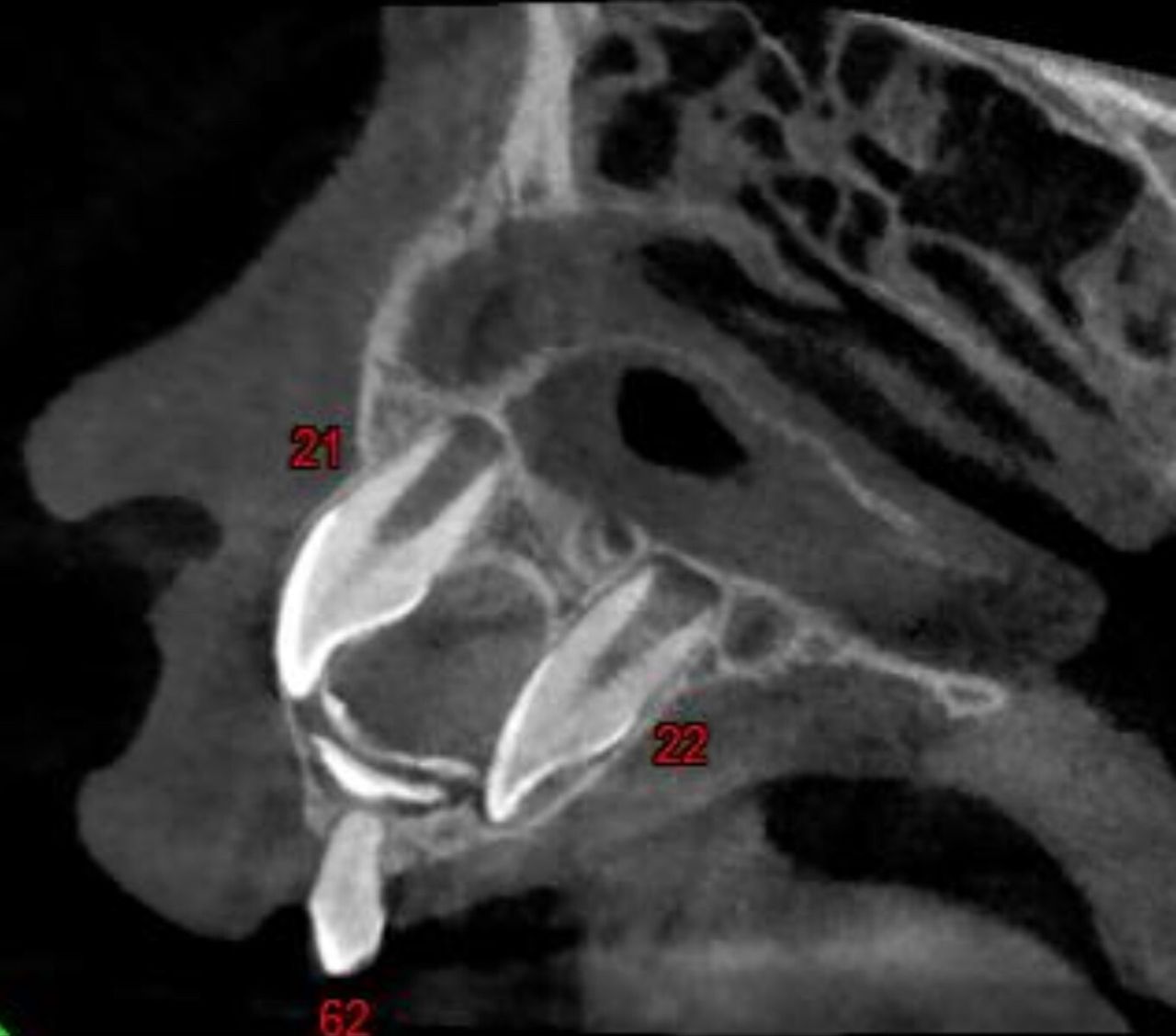
This is a case of a patient in middle childhood in the mixed dentition stage who reported to the hospital with a unerupted permanent tooth in the upper left front tooth region. Parents reported a history of a fall 2 years ago, with no loss of teeth due to the trauma. No abnormalities were detected on examination extraorally. A soft fluctuating swelling was noted intraorally in relation to right primary anterior teeth region on the labial aspect with presence of vestibular obliteration and the presence of a retained primary anterior incisors and no fluid discharge. The cone beam CT image revealed and contributed to localisation of the presence of a well-defined radiodensity similar to that of enamel and dentin arranged haphazardly simulating that of a partially formed crown structure, at its greatest dimension measuring approximately 7.8 mm×9.6 mm anteroposteriorly and mesiodistally and an approximate height of 5 mm from the crest of the alveolar bone to the tip of the coronal structure with a presence of well-defined hypodensity surrounding the structure, with the entire pathology measuring 18 mm×14 mm at its greatest dimension suggestive of cystic changes (figures 1–3). Cystic changes noted involving the cusp of the buccally placed upper left central incisor. Obstruction of the eruption of the permanent teeth was noted due to the presence of the pathology present centrally within the bone and causing displacement of the central incisor buccally and the lateral incisor palatally (figures 4 and 5). Radiographically, a differential diagnosis of a complex odontome near the periapex of retained upper incisors with cystic changes causing obstruction of tooth buds of permanent incisors, a dentigerous cyst arising from permanent left central incisor with the presence of a complex odontoma underneath and a cyst associated with morphologically altered supernumerary tooth was considered. An excisional biopsy (figure 6A–C) was carried out, with the pathology showing histopathological features of densely collegenous connective tissue resembling the dental papilla with small hyperchromatic slanting cells and a surrounding area of reduced enamel epithelium with a few odontogenic cell rests, in some areas forming enamel matrix with dentinal tubules was noted, the decalcified sections showing dentinal tubules and scalloping of one end with pulpal tissue at the other end (figure 7A–D). Thus, correlating histopathologically, radiologically and clinically, the final diagnosis provided was that of abortive tooth formation of a supernumerary tooth.
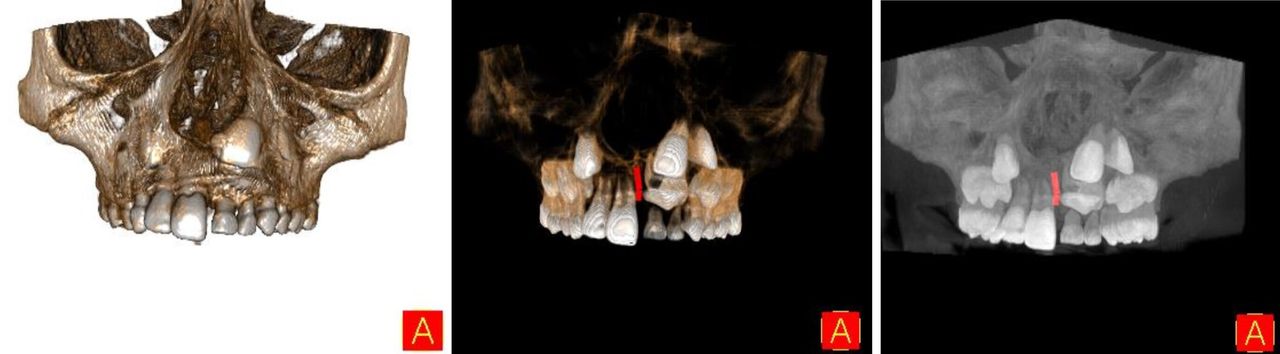
A three-dimensional volume rendered technique reconstruction of the maxilla.

Three-dimensional reconstruction of the maxilla, seen in the axial section.

Panoramic reconstruction of the image.

Axial view of the pathology.
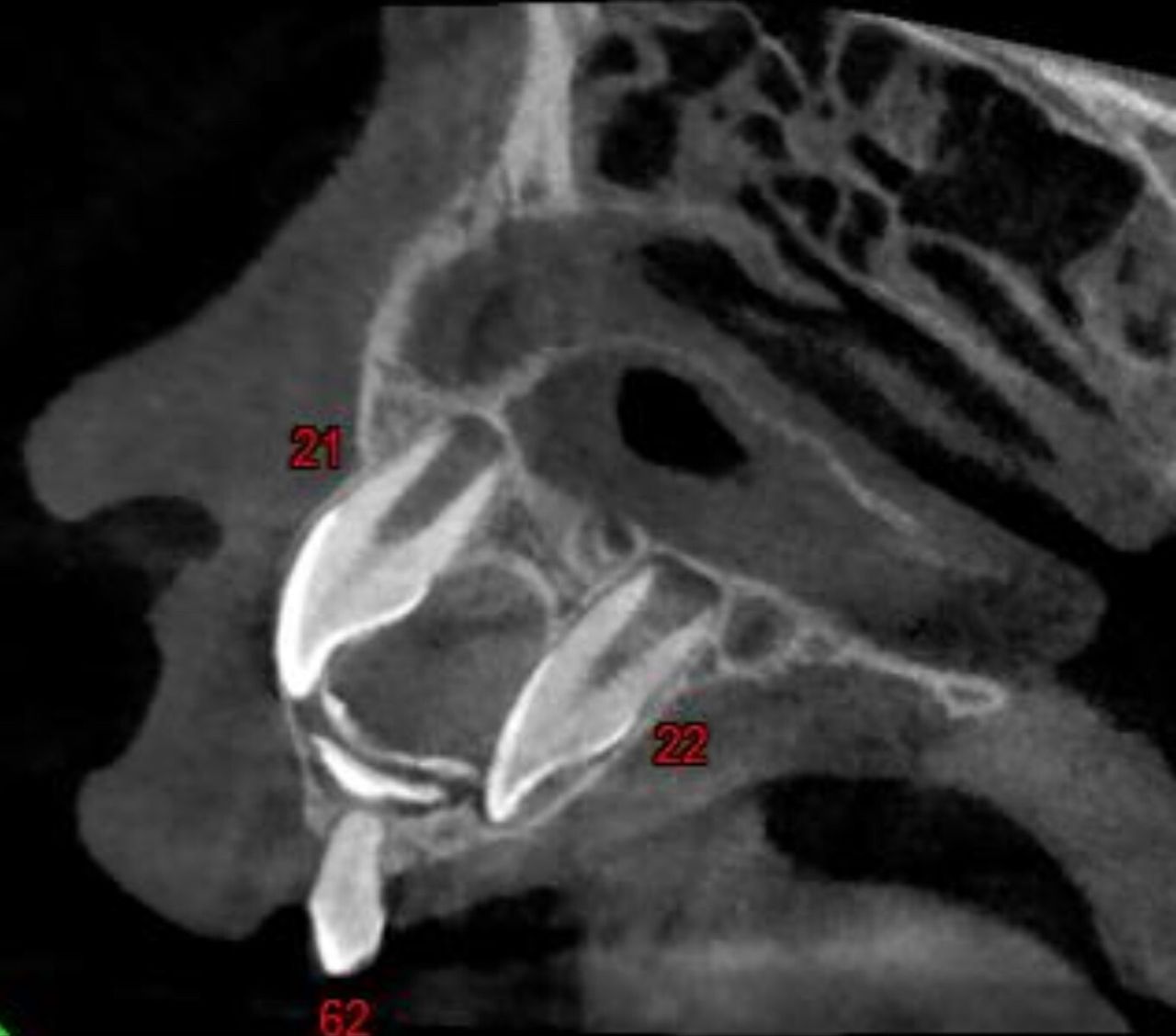
Sagittal view of the pathology.

(A–C) Operative view of pathology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) View of specimen (B) photomicrographs—low power view of the specimen showing presence of enamel matrix, dentin and collagenous tissue resembling dental papilla (C) photomicrograph —high power view of the specimen showing presence of enamel matrix and dentin (D) photomicrograph—decalcified section showing presence of dentinal sheath and tubules.
Supernumerary teeth in primary dentition usually appear conical in shape, while those which occur during permanent dentition may either appear to be miniature, rudiments or have varying other appearances. The presence of an over active dental lamina leads to the formation of supernumerary teeth. While some supernumerary teeth appear to be impacted with no adverse effects, others may cause a broad range of complications like delayed eruption, of permanent teeth, resorption of the root, periodontal lesions, pulpal necrosis and also in some cases cause the formation of dentigerous cysts.1 Trauma also plays a role in the delayed eruption of teeth which has been reported by various authors. Children and adolescents are prone to dental trauma due to play or accidents at school.2 Andersson reported that there is a 20% prevalence of traumatic dental injuries (TDIs) among children and adolescents.3 Petti et al found that TDIS occur in both primary and permanent dentitions, although the prevalence in primary dentition is higher. Prevalence differs with age and sex, with a global male-to-female ratio of 1:43, suggesting that men are more likely to develop TDIs than are women.4 TDI in primary dentition can affect the development of permanent teeth. Damage and/or disturbances to permanent teeth and germs, depending on the mouth area affected, can range from mild to severe. TDI in permanent teeth can cause permanent complications, such as pulp necrosis and internal and/or external root resorption, and influence maxillofacial development which most commonly occurs in the anterior maxilla.2 It is rather unusual to have multiple pathologies in the same region, that is, the presence of an abortive tooth formation, cystic degeneration and clinically as well as radiographically masking the presence of the permanent incisor, where post-trauma, the patient reported delayed eruption of the permanent anterior teeth and the presence of a swelling in the region. Literature most commonly reports fractures of teeth, resorption of the roots and other odontogenic pathology including formation of supernumerary teeth post-TDI, our case is unique in that it reports a case of a multifactorial aetiology, viz., the presence of an overactive dental lamina causing a rudimentary appearance of a supernumerary tooth, and the history of trauma reported by the patient causing the incomplete formation of the supernumerary tooth with the presence of a maxillofacial cystic pathology associated with the tooth which prevented the eruption of the permanent incisors by causing the displacement of the permanent lateral incisor palatally and the central incisor buccally. Thus, based on similar presentation, a radiographic diagnosis of abortive tooth formation of a supernumerary tooth could also be considered.
Patient’s perspective
Patient’s parent:
We did not know that trauma could have such a major impact especially on teeth.
The use of an advanced imaging modality in accurately diagnosing the problem and assessing the depth of invasiveness in removal of the lesion which is a major advantage.
Learning points
This is a unique presentation of tooth post-trauma.
Trauma during the paediatric age group can have adverse effects on the developing dentition, especially during the morphodifferentiation stage.
While most teeth post-trauma are accompanied by fractures of the tooth, resorption of the root or in some cases, maxillofacial pathology—in this case, it is noted that the supernumerary tooth was not formed completely and instead was associated with enlargement of the dental follicle causing an enlarged follicular space or hyperplastic follicular space.
Ethics statements
Patient consent for publication
Footnotes
Contributors AMS contributed to the manuscript’s planning, content and editing. RSV contributed to the manuscript’s planning, content and reporting. PKN contributed to the reviewing and editing of the manuscript. RJ contributed to the reviewing and editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.