Article Text

Statistics from Altmetric.com
Description
A woman in her late 50s with chronic kidney disease stage V, diabetes mellitus type II, chronic obstructive pulmonary disease (COPD), coronary artery disease and heavy tobacco use presented with altered mental status, hyperkalaemia and mixed respiratory and metabolic acidosis. Physical examination revealed numerous thick hyperkeratotic plaques measuring 10–20 mm located on the forearms and shins with firmly adherent scales over fingers and toes bilaterally with pinpoint capillary bleeding indicative of positive Auspitz sign, in addition to perioral scaly erythematous rash (figures 1 and 2). Her skin lesions initially started 9 months prior to her current presentation. She was treated with triamcinolone 0.1% cream two times per day, which was changed to clobetasol ointment 0.05% two times per day with no significant response. Her altered mental status was attributed to an acute exacerbation of COPD. She was started on intravenous methylprednisolone three times a day as part of the management of COPD exacerbation and hydrocortisone 1% ointment two times per day for dermatitis with no significant improvement of her skin lesions. Histopathological examination of her skin biopsies demonstrated an irregularly acanthotic epidermis with slight spongiosis, psoriasiform epidermal hyperplasia, perivascular lymphocytic infiltration, hyperkeratosis and confluent parakeratosis with neutrophilic collections (figures 3 and 4). A preliminary diagnosis of rupioid psoriasis versus acrokeratosis paraneoplastica was made. There was a concern for a potential underlying internal malignancy given the classification of acrokeratosis paraneoplastica a paraneoplastic dermatosis. She had a family history of type 2 diabetes, breast and colon cancer, asthma, COPD and coronary arterial disease. Therefore, CT of the chest and abdomen and esophagogastroduodenoscopy was performed with negative findings for any underlying neoplasia. A final diagnosis of rupioid psoriasis was made and due to the lack of response to topical and systemic steroids, she was started on 0.1% tacrolimus cream applied to bilateral upper and lower extremities two times per day with significant improvement of her skin lesions within 2 days. Unfortunately, after hospital discharge, she was lost to follow-up.

(A–F) Hyperkeratotic plaques measuring 10–20 mm located in hands, forearms, elbows, toes and toenails.

(A–C) Hyperkeratotic plaques measuring 10–20 mm located in the shins and thighs with pinpoint capillary bleeding indicative of positive Auspitz sign.
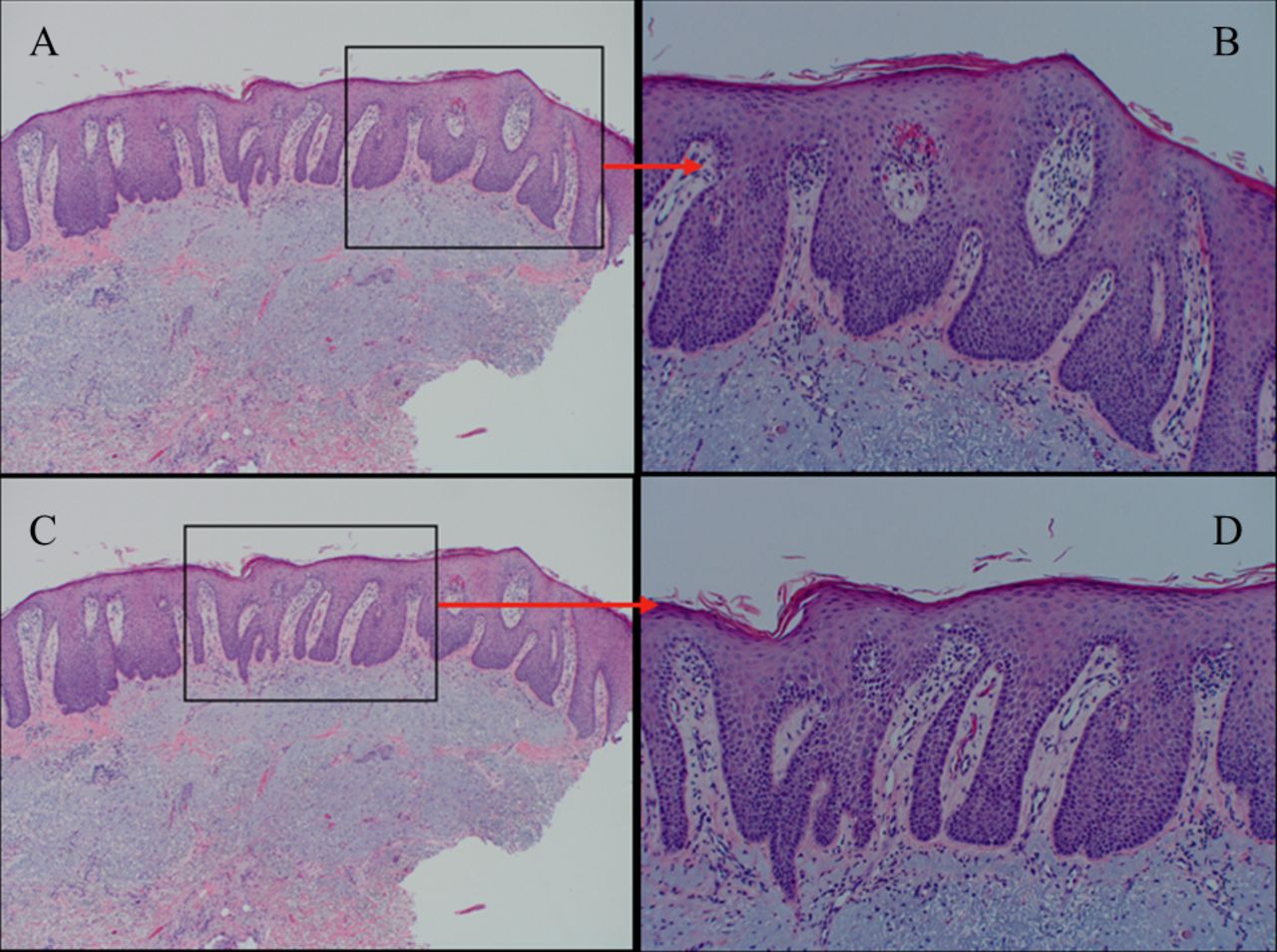
(A–D) Histopathology sections stained by (H&E) illustrating irregular acanthosis, psoriasiform epidermal hyperplasia, hyperkeratosis, parakeratosis and perivascular lymphocytic infiltrate. There is no focal vacuolar interface dermatitis nor mucin. (H&E-stained image at ×10 magnification (left-sided panels) and ×20 magnification (right-sided panels)).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histopathology section illustrating confluent plate-like parakeratosis with small neutrophilic collections (H&E-stained image at ×10 magnification).
Rupioid psoriasis, a subtype of plaque psoriasis characterised by circular or oval-shaped crusted lesions resembling an oyster shell, can be triggered by certain medications including lithium, beta-blockers and synthetic antimalarials or in association with HIV.1 2 Other conditions that may present with similar cutaneous manifestations include syphilis, scabies, sarcoidosis and disseminated histoplasmosis.3 Extracutaneous disorders associated with psoriasis include metabolic syndrome, obesity, chronic kidney disease, COPD, smoking and diabetes mellites, most of which were present in our patient.4 Treatment options for rupioid psoriasis include systemic therapy such as steroids, cyclosporine, methotrexate or biologics combined with intralesional or topical steroids.5 Acrokeratosis paraneoplastica, also known as Bazex syndrome, is a rare paraneoplastic condition characterised by violaceous erythematous rashes and psoriasiform scales that are most prominent in acral sites. Eventually, in the advanced stages, psoriasiform plaques can extend centripetally affecting both extremities and the trunk.6 Acrokeratosis paraneoplastica is usually associated with squamous cell carcinoma of the aerodigestive tracts, especially in the initial stages when a tumour is not apparent. Histopathology findings can be non-specific including hyperkeratosis, parakeratosis, spongiosis and perivascular infiltration as in our case. Unlike rupioid psoriasis, lesions are resistant to targeted therapy such as steroids and improve after treatment of underlying malignancy.7 Making a diagnosis and subsequent treatment can be challenging, as both diseases exhibit non-specific histopathological findings and overlapping cutaneous manifestations.8
Learning points
Rupioid psoriasis may present with non-specific skin biopsy findings of hyperkeratosis, parakeratosis, spongiosis and perivascular infiltration. These cutaneous findings are not to be confused with the cutaneous manifestations of paraneoplastic dermatoses, which can present similarly.
Rupioid psoriasis is a subtype of plaque psoriasis triggered by certain medications, HIV infection, secondary syphilis, scabies and disseminated histoplasmosis.
A key differentiating feature between rupioid psoriasis and acrokeratosis paraneoplastica is that rupioid psoriasis responds to treatment with steroids, methotrexate or biologics with or without topical steroids. Recognising the clinical presentation of paraneoplastic dermatoses can aid in the earlier diagnosis of internal malignancies.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Dr Michelle Tarbox for her help in patient management and interpretation of histopathology images.
Footnotes
Twitter @M_H_Abdelnabi
Contributors AC, JB, CM and MA shared in writing and revising the manuscript. All the authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.