Article Text

Statistics from Altmetric.com
Description
A woman in her 80s was presented to the neurosurgery department with lower back pain aggravated by standing and relieved with rest. She had a medical history of osteoporosis. Mechanical back pain was considered and an osteoporotic lumbar (L1) vertebral compression fracture was verified by MRI and CT (figure 1). It was decided to perform percutaneous vertebroplasty (PV). A 4 mL of polymethylmethacrylate bone cement was injected into the thoracal (T10) vertebral body and 2 mL into the thoracal (T1) and lumbar (L2) vertebral body with fluoroscopic guidance. No complications developed during the procedure. Two days later, the patient had right-sided non-pleuritic chest pain and dyspnoea. Blood gas analysis was normal, she was haemodynamically stable and transthoracic echocardiography showed normal cardiac chambers. Cement embolisation (CE) to pulmonary vessels was suspected. Thorax CT without intravenous contrast administration was performed due to the patient’s contrast allergy. Segmental and subsegmental pulmonary CE and accompanying consolidation and pleural effusion were seen in the right lung on CT (figure 2). In addition, thorax CT demonstrated the cement leaking from the T10 spine into the vertebral venous plexus (figure 3) and reaching into the right pulmonary arterial circulation through the azygos vein (figure 4). Symptomatic therapy was started with intravenous analgesics and supplemental oxygen. Anticoagulation was not initiated as the patient had normal oxygenation and there was no focal filling defect in the main pulmonary arteries. Transoesophageal echocardiography ruled out a source of embolisation from the heart. Symptomatic therapy allowed complete resolution of her complaints and she was discharged after 1 week of hospital stay. Regression of lung findings was observed on the control lumbar CT taken 2 months later (figure 5).
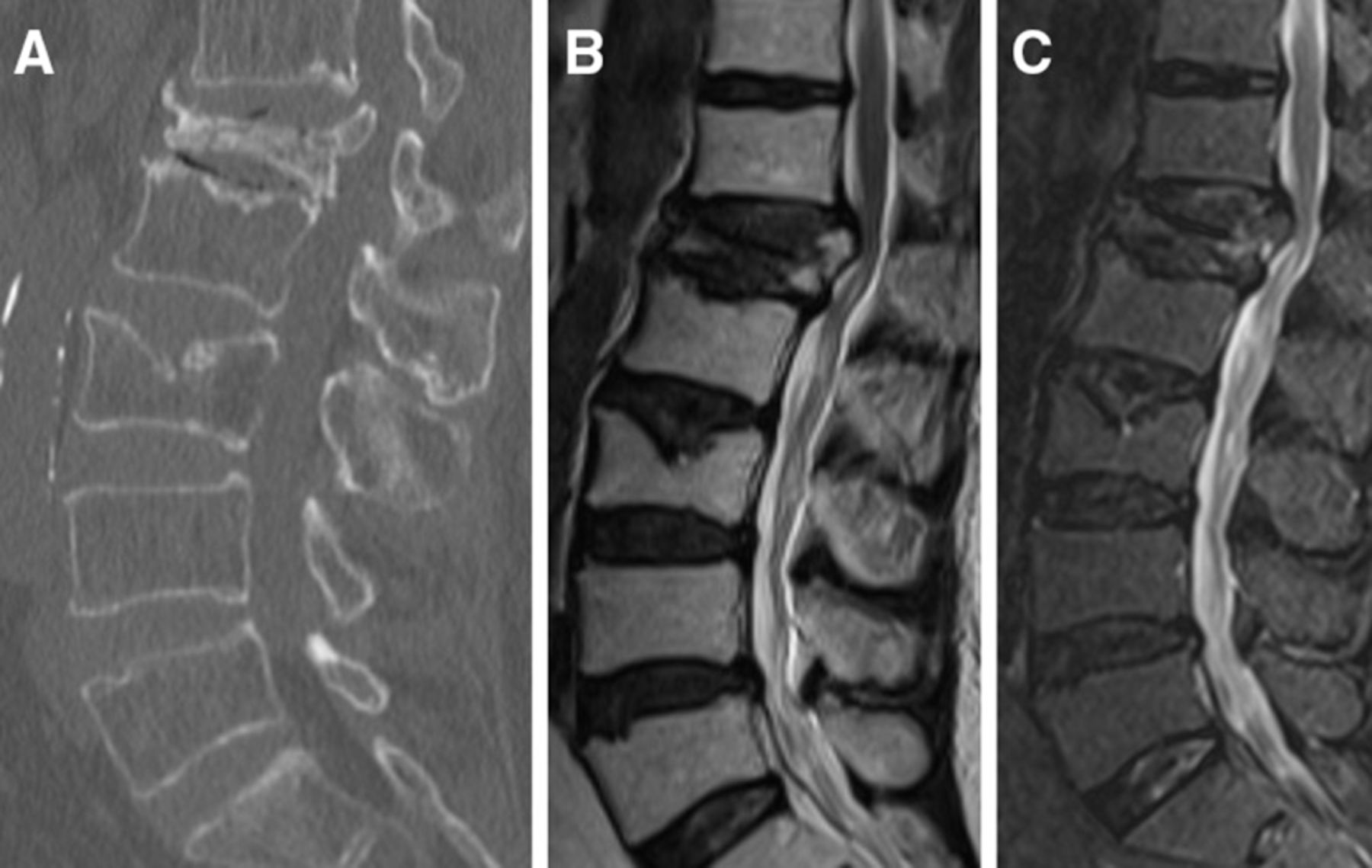
CT (A) and MRIs (B, C) showed lumbar (L1) vertebral body compression fracture.

A preoperative thorax CT image performed for another reason revealed normal imaging findings (A, B). Postoperative thorax CT without intravenous contrast administration demonstrated segmental and multiple subsegmental pulmonary cement embolisms and accompanying consolidation and pleural effusion in the lower and middle lobes of the right lung (C, D).

Axial (A, B) and sagittal (C–E) CT images of the thorax showed the cement leaking from the t10 spine linearly into the vertebral venous plexus (A, C, D; white arrow) and reaching into the right pulmonary arterial circulation through the azygos venous system (B, E; black arrow).

A coronal CT image of the thorax revealed a pulmonary cement embolism (white arrow) and cement in the azygos vein (black arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Control lumbar CT images taken 2 months later demonstrated regression of lung findings and cement still persisting in the azygos vein (A, B; black arrow).
PV is a minimally invasive procedure and is used in the treatment of osteoporotic vertebral compression fractures and osteolytic spinal metastases.1 Polymethylmethacrylate bone cement is injected into the vertebral body by using a transpedicular or paravertebral approach, under fluoroscopic or CT guidance.2 Pulmonary CE may occur as a complication of this procedure with an incidence of 0.9%–23%.3 4 It is caused by the extravasation of cement to the external vertebral venous plexus and later to the azygos vein, vena cava, right heart and finally pulmonary arteries.5 The lung can generally tolerate it without symptoms because the leakages are usually small and cause small CE.6 However, a large cement leakage can cause a pulmonary infarction or even death.6 Patients typically present with symptoms weeks or months after the procedure, but cases presenting immediately or years after the procedure have also been reported.7 This is because inferior vena cava foreign bodies such as intravenous cement can serve as a potential nidus for thromboembolism at any time.8 The risk factors for pulmonary CE include PV procedure, thoracic vertebra treatment, higher cement volume injected per level, more than three vertebrae treated per session and venous cement leakage.1 While treatment and follow-up are not recommended for asymptomatic patients with peripheral CE, surgical treatment with embolectomy is advised for symptomatic central embolism.4 In addition, the standard treatment of pulmonary thromboembolism, including heparinization and warfarin therapy is suggested for asymptomatic central embolisms or symptomatic peripheral embolisms.4 5 Based on the present case’s request and stable clinical symptoms, only symptomatic therapy was applied. It was observed that only symptomatic therapy could be an alternative approach for symptomatic peripheral embolisms.
Learning points
Pulmonary cement embolism may occur as a complication of percutaneous vertebral augmentation procedures. It is often asymptomatic but can cause pulmonary infarction and even death.
Routine chest X-ray after vertebroplasty may be helpful for early detection. However, control CT scans should be performed after the procedure for patients with indicative symptoms of pulmonary embolism and/or those in which large cement leakage is detected during the procedure. Even though these may not alter the management of the asymptomatic patients, it should be kept in mind that IVC foreign bodies such as intravenous cement can serve as a potential nidus for thromboembolism at any time.
Standard treatment guidelines for pulmonary thromboembolism are suggested for symptomatic peripheral cement embolisms but it was observed that only symptomatic therapy could be an alternative approach as experienced in the present case.
Ethics statements
Patient consent for publication
Footnotes
Twitter @CTaslicay
Contributors MS, ISM and CAT were involved in the patient’s care including diagnosis, drafted the manuscript and designed the figures. CAT and FSB contributed to drafting the manuscript and revising it critically for important intellectual content. All of the authors declare that they have all participated in the design, execution, and analysis of the paper and that they have approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.