Article Text

Abstract
A full-term infant developed stridor, respiratory distress and hypercarbia shortly after birth requiring urgent airway intervention. The patient underwent urgent intubation via rigid bronchoscopy. The diagnosis of congenital subglottic cyst was made. The cyst was decompressed and the patient was extubated the following day. On repeat laryngoscopy 1 month later, there was no residual disease and the patient remained symptom free. Congenital subglottic cysts are extremely rare and the diagnosis can be either missed or misdiagnosed with more common causes of stridor, such as laryngomalacia. Subglottic cysts may cause total airway obstruction and even death if they are large enough and not treated immediately.
- Anaesthesia
- Ear, nose and throat
- Congenital disorders
- Otolaryngology / ENT
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Congenital subglottic cysts are an exceedingly rare cause of neonatal stridor. Subglottic cysts are almost always an acquired pathology with formation thought to result from mucosal tissue damage and obstruction of mucous glands. Consequently, subglottic cysts tend to be seen in premature infants with a history of tracheal intubation and ventilatory support. A review of the literature revealed very few case reports of congenital subglottic cysts, none of which presented with immediate airway compromise.1 2 The presence of stridor in a newborn should raise suspicion for a congenital airway abnormality, and an urgent evaluation via nasendoscopy should be considered.
Case presentation
The presented case is a full-term infant, born via non-elective caesarean section following a failed induction of labour, for intrauterine growth restriction. APGAR scores were 8 and 8, and the birth weight was 2730 g (<10th centile). The infant developed progressively worsening stridor, respiratory distress and hypoxaemia (desaturation to 60%) over the first hour of life. Treatment was initiated at the maternity hospital, with nasal CPAP (continuous positive airway pressure) at 6 cm H20 and fractional inspired oxygen (FiO2) of 21%. A nasogastric tube was inserted. Despite this therapy, there was a progressive respiratory compromise and the infant was transferred to a tertiary paediatric hospital for urgent evaluation by Ear, Nose and Throat (ENT) specialists.
On examination, significant initial findings included tachypnoea with a respiratory rate of 70 breaths/min, biphasic stridor, a weak cry and an increased work of breathing as evidenced by intercostal recession, and tracheal tug. A venous blood gas demonstrated a respiratory acidosis with a pH of 7.1 and a partial pressure of carbon dioxide (PaC02) of 75 mm Hg, despite an escalation of respiratory support. Fibreoptic nasendoscopy performed on arrival in the neonatal intensive care unit (NICU) by the ENT surgeon demonstrated a normal larynx with a large subglottic mass, causing a near complete occlusion of the trachea.
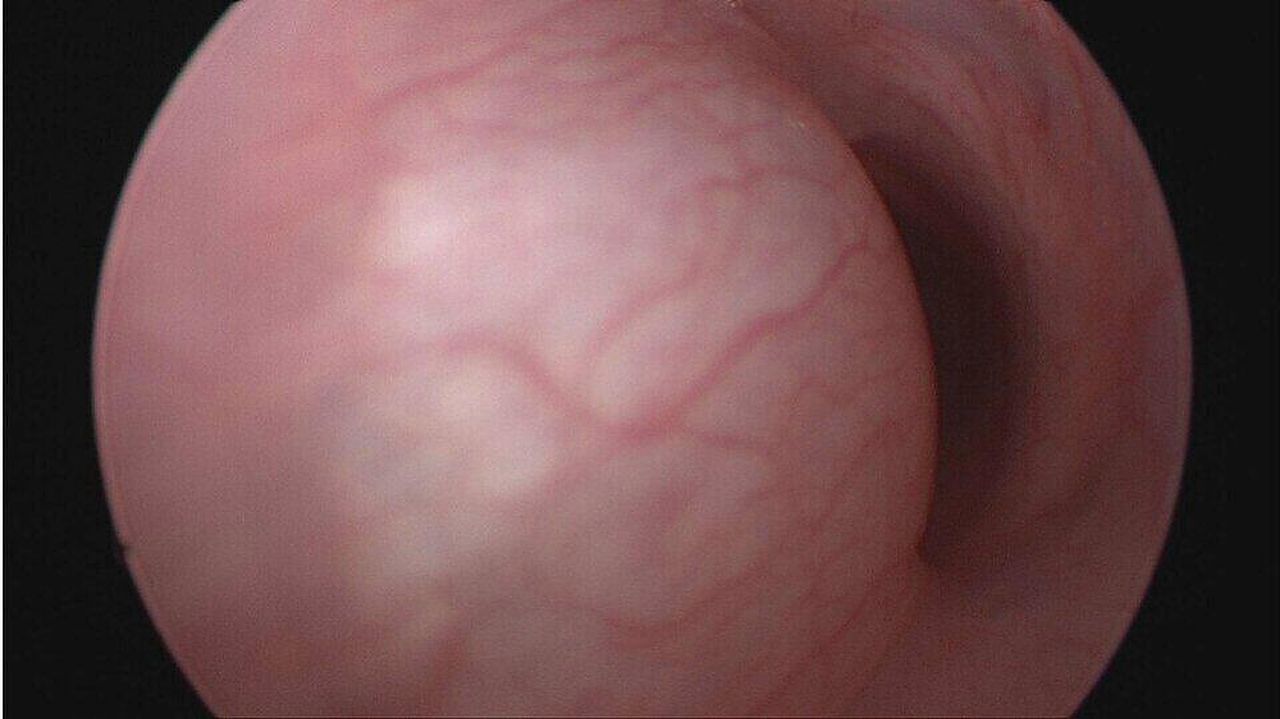
An urgent transfer to theatre was planned for this infant to facilitate tracheal intubation. A pre-procedure plan was formulated by the anaesthesia and ENT teams, with a tracheostomy tray opened and placed on stand by in theatre. On arrival in the operating room, nasal high-flow humidified oxygen was applied, at a flow rate of 5 L/min (2 mL/kg), and an FiO2 of 1.0. Anaesthesia was induced using an intravenous technique. A second intravenous line was inserted, and anaesthesia was maintained with an intravenous propofol/ketaminel infusion (10 mg/mL propofol/1 mg/mL ketamine), and supplemented with additional ketamine boluses of 0.5 mg/kg as required. Depth of anaesthesia was titrated to tolerate instrumentation of the airway while maintaining spontaneous ventilation throughout the case. The airway was initially visualised using a video laryngoscope (Storz CMAC) fitted with a Miller 1 laryngoscope blade, and topicalised using 1 mL of 1% lidocaine via an atomiser device. On rigid bronchoscopy, a view of the subglottis demonstrated a large left-sided posterolateral subglottic cyst, occluding more than 90% of the airway (figure 1). Intubation was performed by the surgeon via rigid ventilating bronchoscopy with a size 2.5 uncuffed endotracheal tube loaded onto a 2.5 mm Hopkins optical rod telescope. After confirmation of successful ventilation, the cyst was then decompressed endoscopically using an endoscopic sickle knife and the airway was suctioned. Betamethasone was injected into the subglottic submucosa. The Hopkins optical rod telescope was then passed to examine the trachea and main bronchi distal to the cyst; no further airway anomalies were identified (video 1). The patient was reintubated with a size 3 cuffed endotracheal tube and transferred back to the NICU for ventilation overnight. The patient was extubated uneventfully the following day and was discharged home on day 5.

{kind=link}
Telescopic view of subglottis demonstrating a large congenital subglottic cyst.
Outcome and follow-up
The infant underwent repeat laryngotracheobronchoscopic examination at 1 month post-discharge, demonstrating no residual pathology. The patient was subsequently followed up 3 months later in the outpatient clinic and remained symptom free.
Differential diagnosis
The differential diagnosis for an infant with stridor should also include laryngomalacia, bilateral vocal fold paralysis, subglottic stenosis, saccular cyst, laryngeal web, tracheobronchomalacia and subglottic haemangioma.
Discussion
Subglottic cysts are retention cysts of subepithelial mucosal glands, which may be either congenital or acquired. Subglottic cysts are rare and occur at a rate of ~1.8/100 000 live births.1 The incidence of subglottic cysts is increasing and is thought to be secondary to the increased survival rates of premature infants. These premature infants frequently require prolonged duration of tracheal intubation (a known mechanism for the formation of acquired subglottic cysts). The mechanism is however not completely understood. Acquired cysts are presumed to be iatrogenic and secondary to repetitive piston trauma of the endotracheal tube and ventilator on subglottic mucosa.2 This may result in the blockage of the subglottic ducts as a result of erosion and subsequent scarring. In contrast, congenital subglottic cysts can occur in term neonates with no previous airway intervention. The subglottic region is the narrowest segment of the paediatric airway, and therefore narrowing secondary to either acquired or congenital subglottic cysts has the potential to cause rapidly progressive respiratory distress and complete airway obstruction.3 4
The non-specific symptoms related to subglottic cysts may present a diagnostic challenge. A high index of suspicion is required to ensure appropriate and timely investigation and treatment. Common symptoms include dysphonia, dysphagia, hoarseness, stridor and dyspnoea. All of which are easier to detect in older children. This condition may be misdiagnosed as laryngomalacia, croup or subglottic stenosis, due to the similar characteristic features and the relative rarity of the congenital subglottic cysts. Diagnostic laryngoscopy and bronchoscopy are therefore routinely indicated for airway evaluation in at-risk infants.5
There are, however, certain features in the history and examination to assist clinicians in differentiating these conditions. Stridor implies a narrowing in a level of the laryngotracheal pathway. Stridor during inspiration suggests obstruction above the vocal cords, in conditions such as laryngomalacia and vallecula cysts. A biphasic stridor is more typical of obstruction at the level of the vocal cords or subglottic, which may be present in conditions such as unilateral and bilateral vocal cord palsy, subglottic stenosis and subglottic cysts. Expiratory stridor is commonly associated with obstruction at the level of the trachea, in conditions such as tracheomalacia, tracheal stenosis and vascular rings.6
Assessing the response to treatment may assist in making the correct diagnosis. A good response to epinephrine and corticosteroids may be seen in inflammatory conditions, such as croup. The use of positive end expiratory pressure or CPAP may show the most improvement in dynamic obstruction, such as in tracheobronchomalacia.6
Laryngomalacia is the most common cause of neonatal stridor and symptoms are often exacerbated during feeding, agitation or when supine. While it may be present at birth, it usually develops in the weeks to months after birth. Most cases of laryngomalacia will self-resolve; however, treatment includes managing reflux and thickened feeds for mild-to-moderate disease and surgical intervention with supraglottoplasty for severe disease.7 In our case, a diagnosis of laryngomalacia was less likely as the stridor was present from birth, biphasic and unchanged with position.
Vocal cord palsy is the second most common cause for neonatal stridor and may be congenital or iatrogenic. Iatrogenic causes include cardiac surgeries and tracheo-oesophageal fistula repair. Unilateral vocal cord palsy usually presents with weak cry and aspiration, but can also present with stridor. Bilateral vocal cord palsy is more likely to result in severe airway obstruction with blue spells and may require urgent tracheostomy.8
Acquired subglottic cysts are often treated with endoscopic marsupialisation with cold steel instruments. CO2 laser, coblation and a microdebrider are used cautiously to avoid creating circumferential scarring of an already narrow neonatal or infant airway. Due to the rarity of the condition, there is no consensus on the treatment of congenital subglottic cysts although the overarching goal remains the same: to establish and maintain a patient airway with resolution of symptoms, minimal residual scarring and no recurrence. In this case report, the priority was focused on urgently securing the airway and restoring airway patency. Fortunately, there was no evidence of recurrence or scarring on follow-up laryngoscopy. While the recurrence rates in congenital subglottic cysts are unknown, recurrence rates in acquired subglottic cyst may be as high as 20%.9 10
Management requires a multidisciplinary team approach. Clear communication, role allocation and an agreed stepwise plan to manage the shared airway, including the need for an emergency tracheostomy in the event of an evolving ‘can’t intubate, can’t oxygenate’ scenario, are paramount. The risk of sudden and severe airway obstruction highlights the need for a prompt diagnosis and management plan coordinated by experienced ENT surgical and anaesthetic teams.11
Patient’s perspective
Looking back at our experience, we are grateful for the expertise and professionalism of those from the hospital. It was obviously a very distressing time, but we knew (he) was in great hands.
Although I couldn’t be at the hospital, I was provided regular updates via phone and involved in decision making and was always aware of all possibilities and potential outcomes.
It’s been a surreal experience that (sic) we hope we never have to experience again- it’s been tough emotionally and mentally especially in the beginning. We worry so much already about SIDS [sudden infant death syndrome] especially as first-time parents, those first few weeks were especially challenging as we were constantly worried that he was going to stop breathing. Our child is now healthy and thriving, we couldn’t thank the team involved in his care enough and modern technology for the treatment and care our child received.
Learning points
Congenital subglottic cysts are rare and can occur in term neonates with no history of airway trauma or intubation.
In neonates with stridor, early referral to an experienced Ear, Nose and Throat surgeon is recommended for direct visualisation of the tracheobronchial anatomy to establish a diagnosis.
A positive perioperative outcome is dependent on clear lines of communication between surgeon, anaesthesiologist and theatre teams.
Contingency plans for an emergency surgical airway must be in place before induction of anaesthesia in the event of total airway obstruction or a ‘can’t intubate, can’t ventilate’ scenario.
Ethics statements
Patient consent for publication
Footnotes
Twitter @SamuelLast11, @DrHeatherIsabel
Contributors SPL participated in the drafting, revising and conception of the manuscript. HIP gave anaesthetic input and was a coauthor. SV and NH participated in the editing and revision of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.