Article Text

Abstract
Sphenoid sinusitis is a clinically important entity as it may be associated with catastrophic complications including cavernous sinus thrombosis (CST), cerebral abscess or infarction, meningitis, base of skull osteomyelitis and cranial nerve palsies. We report a case of occult sphenoid sinusitis presenting as Streptococcus intermedius bacteraemia, bilateral jugular vein and CST, cranial nerve palsy and base of skull osteomyelitis.
- Ear, nose and throat/otolaryngology
- Infectious diseases
- Cranial nerves
- Haematology (incl blood transfusion)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Ear, nose and throat/otolaryngology
- Infectious diseases
- Cranial nerves
- Haematology (incl blood transfusion)
Background
The sphenoid sinus is the most posterior paranasal sinus. It is formed as a pair of spaces within the sphenoid bone. Superiorly and posteriorly, it is related to the sella turcica and laterally by the cavernous sinus and middle cranial fossa. Sphenoid sinusitis may lead to devastating complications with contiguous involvement of the cavernous sinus and its contents, including the internal carotid artery and cranial nerves III, IV, V and VI.1 2 Management of sphenoid sinusitis includes antimicrobials, intranasal corticosteroids and topical decongestants. If medical management is unsuccessful, surgical intervention can be considered.1 Functional endoscopic sinus surgery is the standard surgical technique used to drain chronic and recurrent sinusitis.3 The role of anticoagulation in sphenoid sinusitis complicated by thromboses, such as cavernous sinus thrombosis (CST), remains controversial.4 A high index of suspicion is required to recognise and manage sphenoid sinus disease before complications emerge. We present a case of a healthy man in his mid-20s with sphenoid sinusitis complicated by epidural abscess and multiple thromboses.
Case presentation
A man in his mid-20s, with a background of type 1 diabetes mellitus, presented with a 4-week history of posterior neck pain, 2 weeks of persistent headaches, 1 week of odynophagia and subjective fevers complicated by 4 days of progressive tongue swelling.
He had previously presented to the emergency department twice prior for headaches and neck pain, however, after normal neck X-ray, non-contrast CT head and clinical review, he was sent home. In retrospect these symptoms were likely related to his subsequent admission with headaches related to sphenoid sinusitis. His medical history was significant for type 1 diabetes, with a recent haemoglobin A1c (HbA1c) of 8.5% and no microvascular or macrovascular complications. He was a non-smoker, social drinker and denied any intravenous and recreational drug use.
On presentation, he was afebrile, normotensive with a respiratory rate of 18 breaths/min, oxygen saturations of 97% of 1 L of oxygen and a heart rate of 107 beats per minute. On initial examination, he had slightly reduced range of movement in his neck, as well as paravertebral neck tenderness around C1–4. He was dysarthric with no other cranial neuropathies. His cardiovascular, respiratory, abdominal and neurological examination were otherwise unremarkable.
On the second day of admission, he developed bilateral tongue weakness, nystagmus on left gaze and right palatial weakness with uvula deviation. He was noted to have a hypernasal voice, as well as developing persistent fevers to 39°C.
Investigations
Initial baseline blood tests revealed and elevated white cell count of 15.1 (4.0–11.0×109/L), neutrophil count 12.26 (2.0–8.0 x 109 /L) and raised inflammatory markers with a C reactive protein of 325 (<5.0 mg/L). Streptococcus intermedius was recovered from blood culture in two of two bottles at 13.4 hours.
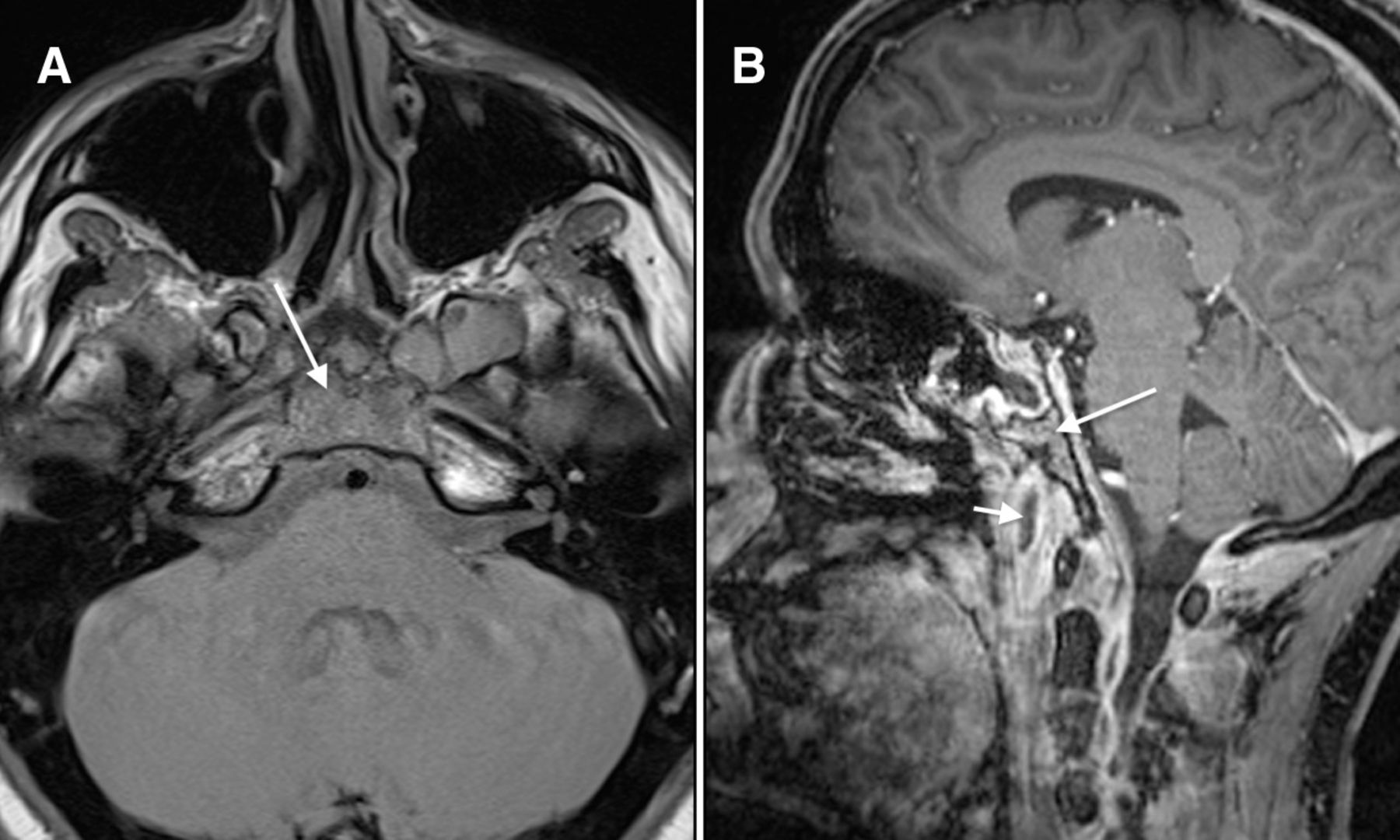
CT with contrast of the head, neck, chest and upper abdomen was performed, which revealed bilateral sphenoid sinusitis (figure 1A) bilateral non-occlusive internal jugular vein thrombosis (figure 1B), CST (figure 1C) and multiple septic emboli within the chest (figure 1D). Transthoracic echocardiography was performed which revealed a structurally normal heart without evidence of infective endocarditis. Contrast-enhanced MRI of the brain and neck revealed an epidural abscess extending from C1 to C4, a large retropharyngeal collection (figure 2A), and base of skull inflammation with associated hypoglossal foramen involvement and suppurative intramuscular collections in the left longus capitus (figure 2B). A serial MRI was repeated after seven days which showed base of skull osteomyelitis, with clival involvement (figure 3A), centred around C0-1 and a peripherally enhancing abscess in the left longus capitus muscle (figure 3B).

(A) Sagittal contrast-enhanced CT of the neck shows a retropharyngeal fluid collection (arrows). (B) Contrast-enhanced CT of the neck shows filling defects in both internal jugular veins (arrows) consistent with thrombus. (C) Contrast-enhanced CT of the brain demonstrates no enhancement within the cavernous sinus on the left (arrow) and patchy enhancement on the right. (D) Contrast-enhanced CT of the chest shows several pulmonary nodules (arrow) consistent with septic emboli to the lungs.
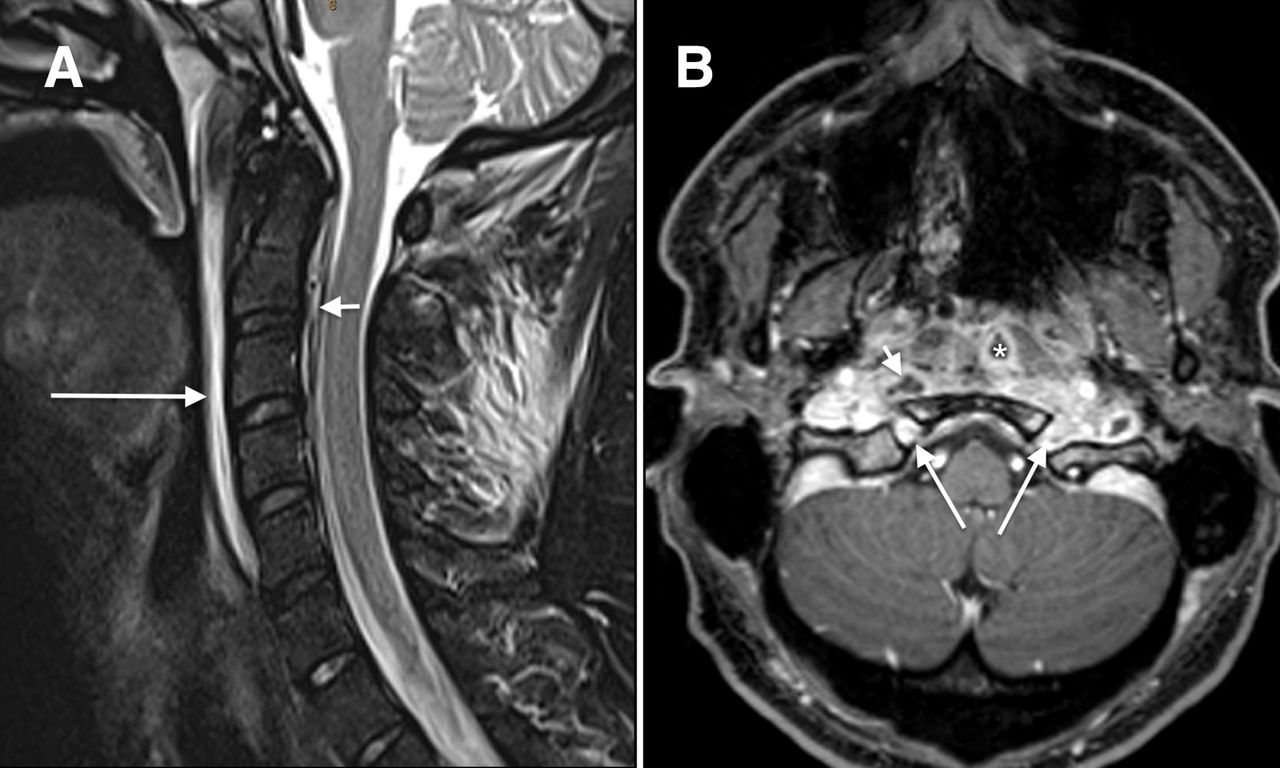
(A) Sagittal T2 with fat saturation shows the retropharyngeal fluid collection (long arrow) and small epidural collection (short arrow). (B) Axial T1 postcontrast with fat saturation demonstrates diffuse abnormal enhancement around the skull base involving the hypoglossal foramen bilaterally (long arrows) with abscess in the left longus capitus muscle (*) and retropharyngeal abscess (short arrow).

{kind=link}
{kind=link}
{kind=link}
(A) Axial T1-weighted MRI demonstrates low T1 signal within the clivus (arrow). (B) Sagittal T1 contrast-enhanced MRI with fat saturation shows abnormal enhancement of the clivus (arrow) consistent with skull base osteomyelitis. The peripherally enhancing abscess in the left longus capitus muscle (short arrow) is also demonstrated.
Differential diagnosis
Lemierre’s syndrome is rare condition characterised by thrombophlebitis of the internal jugular vein, bacteraemia and pulmonary septic embolisation as a consequence of oropharyngeal infection.5 6 It is typically caused by Fusobacterium necrophorum and affects young healthy adults with the median age of patients between 19 and 22 years old and a 2:1 male to female ratio.7 However, Lemierre’s syndrome is classically preceded by pharyngitis, which was absent in this case and the development of bilateral jugular thrombosis (as seen in this case) is atypical, although reported.8
Treatment
A single 8 mg dose of intravenous dexamethasone was administered due to concerns of deep neck space infection. Intravenous piperacillin-tazobactam 4.5 g four times per day was commenced and rationalised to ceftriaxone 2 g ntravenous daily when microbiology results were available. Consultations from otolaryngology, head and neck surgery, neurosurgery, orthopaedics were sought, however, surgical intervention was not required in this case. Therapeutic anticoagulation was implemented. The initial heparin bolus dose was 1450 units, followed by a heparin infusion with the patient’s rate varying between 2100 units/hour and 2360 units/hour, titrating to an activated partial thromboplastin time (APTT) between 65 and 100. Over the following week, there was clinical improvement, and he was discharged on day 12. He received intravenous ceftriaxone for a total 6 weeks, followed by oral amoxycillin 1 g four times per day for 3 months. Anticoagulation was continued with subcutaneous enoxaparin 80 mg two times per day for 4.5 weeks, followed by rivaroxaban 20 mg orally once daily for 12 weeks.
Outcome and follow-up
Three days postdischarge, the patient represented for right-sided pleuritic chest pain and computed tomographic pulmonary angiogram (CTPA) revealed scattered subsegmental pulmonary emboli. Repeat blood cultures were negative. He was discharged after confirmation that his anti-Xa levels were within therapeutic range. An MRI was performed at 1 month, which demonstrated improvement of sphenoid sinusitis and resolution of the epidural abscess, intramuscular abscess and CST. He reported no further symptoms and cranial nerve examination was normal.
Discussion
Here, we present a case of occult sphenoid sinusitis in a young male presenting with Streptococcus milleri blood stream infection, base of skull osteomyelitis resulting in cranial nerve IX and XII palsies, retropharyngeal and epidural abscess, cavernous sinus and bilateral jugular thrombophlebitis and septic pulmonary emboli. Our case had full resolution of symptoms after a 4-month course of antibiotics and anticoagulation. The sequence of events likely began with sphenoid sinusitis, with subsequent contiguous infection of surrounding anatomy including cavernous sinus and jugular veins, resultant endovascular infection and bacteraemia. Furthermore, endovascular infection of the jugular vein and cavernous sinus likely acted as potent stimulators for thrombosis, via release of prothrombotic factors and indirectly from tissue damage secondary to toxins.9
Sinusitis is defined as the inflammation of the paranasal sinuses and may be classified as acute or chronic, where chronic sinusitis involves symptoms for 12 weeks.1 Typical pathogens, accounting for more than half of the cases, are Streptococcus pneumonia and Haemophilus influenzae.10 Streptococcus milleri group are commensal oropharyngeal organisms, which are a less common cause of sinusitis and associated with head and neck abscesses.1
Less than 3% of inflammatory lesions of the sinuses primarily involve the sphenoid sinus, with the sphenoid sinus being historically referred to as the ‘neglected sinus’.11 12 Isolated sphenoid sinus disease is rare and refers to unilateral cases.
This case illustrates the significant diagnostic challenge presented by sphenoid sinusitis, due to its anatomical location and non-specific early symptoms.13 In some cases of isolated sphenoid sinus disease, the early stages are asymptomatic.5 The most common presenting symptom is headache, mainly in the retro-orbital and frontal areas.2 In this case, the patient presented on two occasions for assessment of headache and opportunity for diagnosis and early intervention was missed. Less common presentations include neck pain, earache and a sore throat and cranial nerve deficits; complications which in our case lead to diagnosis.10 11 Acute, uncomplicated sphenoid sinus disease may be treated conservatively with broad-spectrum antimicrobials and nasal decongestants.6 The goals of surgery are to decompress the sphenoid sinus by establishing drainage, potentially avoiding later complications and to obtain material for microbiological culture. Surgical intervention should be considered in cases that fail to respond to conservative therapy or develop complications.7 In this case, multidisciplinary surgical consultation was sought at presentation, however, after a period of close observation, surgery was avoided.
The use of a single dose of glucocorticoid in cervico-facial infections is widespread. Some indications (pharyngitis, peritonsillar abscess, sore throat) have been examined and are supported through randomised controlled trials while further evaluation is required for other indications.8 14
Anticoagulation for aseptic CST is well defined, however, the use is not generalisable to septic cases, due to the differing pathophysiology of the thrombosis.15 There are currently no randomised controlled trials to guide the decision on anticoagulation for septic CST and prospective trials would be impractical to recruit due to the rarity of the condition.16
In a literature review Caranfa and Yoon cited a number of theories supporting anticoagulation including anti-inflammatory benefits, prevention of thrombi extension and allowing the antibiotic to penetrate the thrombus.9 Conversely, some authors argue that the possibility of fragmentation of fresh embolus may lead to new septic emboli and should give caution to the use of anticoagulation.17
A review of the literature by Weerasinghe and Lueck reports 41 out of 88 patients receiving anticoagulation. Here, a wide variety of anticoagulants with differing durations were described. The majority received 2–6 weeks, however, five patients were anticoagulated for 3 months or more. 53.26% made a complete recovery in the anticoagulated group compared with 32% who were not anticoagulated. Furthermore, mortality was much lower in the anticoagulated group 28% vs 12%.18 However, fatal subarachnoid haemorrhage occurring within 24 hours of initiation of low-molecular-weight heparin, in a case of CST due to ipsilateral sphenoid sinusitis, serves as a timely reminder of the risks of systemic anticoagulation.15
Our case was managed conservatively with high-dose antibiotics and therapeutic anticoagulation, with complete resolution of symptoms.
Learning points
Sphenoid sinusitis can have life-threatening complications necessitating aggressive medical management and consideration of surgery. A high index of suspicion is required for diagnosis.
Anticoagulation for septic cavernous sinus thrombosis remains a controversial topic with initiation and duration guided by individual cases, including ongoing prothrombotic factors and bleeding risk.
Conservative therapy is recommended as initial management, however, surgical intervention may be required if there is failure to respond or the development of complications.
Ethics statements
Patient consent for publication
Footnotes
Twitter @drjengillespie
Contributors WJ, TS and PC were responsible for the clinical care of the patient. WJ and TS contributed equally to the preparation of the manuscript. PC and JG edited the manuscript and contributed to the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.