Article Text

Statistics from Altmetric.com
Description
A man in his 40s with a significant urological history of neurogenic bladder after blunt abdominal trauma status post-suprapubic catheter complicated with recurrent urinary tract infections (UTIs) presented with a 2-week history of dysuria, haematuria and flank pain. He denied any fever or chills, nausea or vomiting. Physical examination revealed right-sided costovertebral angle tenderness with an ill-defined mass. His laboratory workup showed leucocytosis with a white cell count (WBC) of 18.6×103/µL with 85% neutrophils and baseline creatinine of 1.7 mg/dL. Urine analysis was cloudy with elevated WBC, red blood cells, positive nitrite and leucocyte esterase. CT of the abdomen and pelvis with intravenous contrast demonstrated a markedly enlarged right kidney with ‘bear paw sign’, multiple, low-density areas suggestive of necrosis or abscess corresponding with xanthogranulomatous pyelonephritis (XGP) (figures 1 and 2). He was started on a piperacillin/tazobactam combination as empirical therapy for UTI. Urine culture grew 100 000 CFU/mL pansensitive Pseudomonas. He was discharged on an oral antibiotic regimen of levofloxacin for 6 weeks and scheduled for a follow-up on an outpatient basis. On his follow-up after completion of antibiotic therapy, he reported total resolution of his symptoms, and an elective right nephrectomy was planned after counselling. XGP is a rare severe chronic inflammatory disease of the renal parenchyma, which is characterised by the destruction of the renal parenchyma and granulomatous inflammation, with lipid-laden foamy macrophages as well as inflammatory infiltration and extensive renal fibrosis.1 Although the aetiology of XGP remains unclear, it is commonly associated with recurrent UTIs and obstructive nephropathy. Other proposed aetiologies include altered immune response, congenital urinary anomalies, lipid metabolism abnormalities, malnutrition and lymphatic blockage.2 XGP might occur in all age groups, but predominantly affects adults. XGP often occurs unilaterally, and bilateral cases are extremely rare, mostly diffuse and occupationally focal.1 Typical clinical manifestations of XGP are fever of unknown origin, abdomen/flank pain, weight loss, anaemia or palpable renal mass.1 Commonly isolated pathogenic bacteria are Escherichia coli, Klebsiella and Proteus. Differential diagnosis of XGP includes a large variety of conditions such as Wilms tumour, renal cell carcinoma, renal abscess, infected renal cystic disease and tuberculosis; therefore, CT scan is essential for diagnosis and preoperative evaluation, but a tissue biopsy is required to confirm the diagnosis, especially in suspected cases.3 XGP can be classified based on CT features to either diffuse or focal. In diffuse XGP, typical CT findings include renal parenchymal destruction, which is replaced by multiple, rounded, low-density areas with enhancing rings arranged in a hydronephrotic pattern and hypoenhanced renal parenchyma, described as ‘bear paw sign’. While in focal XGP, CT frequently shows a well-defined hypoattenuated localised intrarenal lesion. Depending on the extent of inflammation, XGP can be classified into three stages: nephric XGP (stage I: confined localised disease to the renal parenchyma), perinephric XGP (stage II: the inflammation extends to the perirenal fat) and perinephric XGP (stage III: the lesion extending into perinephric spaces).4 5 The standard management is antibiotic therapy and total nephrectomy, but focal XGP can be treated with antibiotics or nephron-sparing surgery.1 3
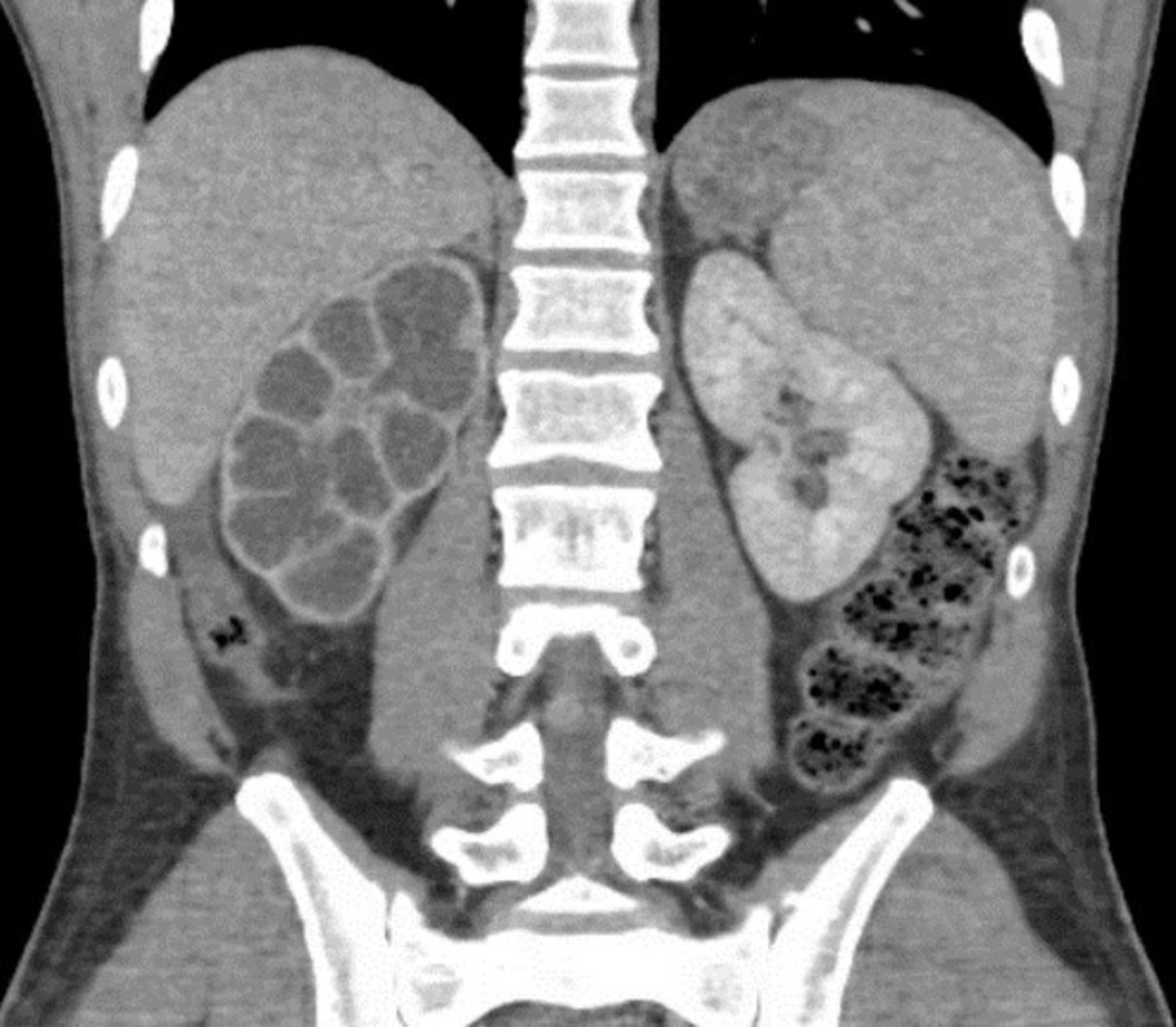
Coronal plane of CT of the abdomen and pelvis showing ‘bear paw sign’: multiple, low-density areas suggestive of necrosis or abscess suggestive of stage II xanthogranulomatous pyelonephritis.

{kind=link}
{kind=link}
Axial plane of CT of the abdomen and pelvis suggestive of stage II xanthogranulomatous pyelonephritis.
Learning points
Xanthogranulomatous pyelonephritis (XGP) is a rare chronic granulomatous inflammation of the renal parenchyma due to recurrent urinary tract infections or obstructive uropathy. Typical clinical manifestations are fever of unknown origin, flank pain or palpable renal mass.
CT of the abdomen and pelvis can establish the diagnosis of XGP, but tissue diagnosis is required to confirm the diagnosis.
The standard management of XGP is antibiotic therapy and total nephrectomy, but partial nephrectomy may be appropriate in select cases.
Ethics statements
Patient consent for publication
Footnotes
Twitter @M_H_Abdelnabi
Contributors MA, AR and MP were involved in patient care. AR and PS wrote the initial draft of the manuscript. MA and MP revised and edited the manuscript. All authors have approved the final submitted manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.