Article Text

Abstract
We present a rare case of microsurgical replantation of a total scalp avulsion. A woman in her mid-60s was renovating a tractor when her hair was caught in a column drill resulting in traumatic scalp avulsion. The avulsed scalp involved the eyebrows and the entire hair-covered part of the scalp. The prehospital management and the conservation packing of the scalp was very effective. Microsurgical replantation was achieved with anastomoses of the left superficial temporal artery and one temporal vein on each side. The combination of the prehospital treatment and our university hospital setup made it possible to reattach the scalp with an ischaemia time of approximately 5 hours. A functional and aesthetically pleasing outcome was achieved, and the patient was discharged 6 days postoperatively with a vital scalp and no complaints. Five months postoperatively, she has no sign of alopecia and is regaining sensation and function of the scalp.
A woman in her mid-60s was renovating a tractor when her hair was caught in a column drill resulting in traumatic scalp avulsion. The avulsed scalp involved the eyebrows and the entire hair-covered part of the scalp. The prehospital management and the conservation packing of the scalp was very effective.
- Trauma
- Surgery
- Plastic and reconstructive surgery
Statistics from Altmetric.com
Background
A total scalp avulsion is a rare and potentially life-threatening injury. Only a limited amount of literature is published on this kind of trauma, mainly case reports or case series.1 2 If possible, microsurgical replantation of the scalp is the preferred treatment.3 4 We wish to share our experience because of the complexity and rarity of this type of trauma. Most of the larger departments of plastic and reconstructive surgery worldwide will have the necessary setup and equipment to perform the procedure. However, only a handful of surgeons will have prior experience with this kind of injury.5
Our aim of this article is to share our experience and thereby provide information that could help others if they are presented with a similar case.
Case presentation
The patient is a female in her mid-60s with no known comorbidities and no daily intake of medicine. She had never been admitted to a hospital previously.
She was renovating a tractor when her hair was caught in a column drill. The high energy pull resulted in a total scalp avulsion including the eyebrows and the entire hair-covered part of the scalp. The upper half of her left ear was only hanging from a thin skin bridge. Fortunately, the patient was able to call for an ambulance. At the scene of the accident, the paramedics packed the scalp very efficiently. First the scalp flap was placed in a plastic bag that was then placed in another plastic bag containing cold water and ice cubes to reduce the metabolism of the scalp. The patient was brought to the trauma center by ambulance. In the ambulance, she was given fentanyl 50 μg two times due to her pain. During transit, the patient was sitting up, alert and awake (figure 1). As seen in figure 1, the traumatic scalp avulsion resulted in haemorrhage. Fortunately, the bleeding had stopped spontaneously when the ambulance arrived. The patient’s head was only covered around her face to protect her eyes from potential rebleeding during transportation to the hospital.

In the ambulance. The patient sitting up awake and alert.
Two hours after the accident, she arrived at the trauma center. She was ABCDE (Airway, Breathing, Circulation, Disability, Exposure) stabile with a blood pressure: 132/64 mm Hg, pulse: 85, saturation without oxygen supply: 95%, respiration rate 22 and GCS (Glasgow Coma Scale) 15.
Investigations
Due to the high energy nature of the trauma, we did a CT scan of her cerebrum, facial bones and cervical spine. The scans showed no sign of intracranial bleeding or fractures.
Treatment
After the initial examination at the trauma center, the patient was transferred to the operating room at the department of plastic surgery. The patient was anaesthetised, and the scalp was unpacked and prepped for surgery (figure 2). The hair was cut short and visible foreign bodies were removed using saline and forceps. All vessels were identified and treated with heparin to avoid thrombosis. The entire circumference of the scalp was revised. The patient’s head was unpacked and washed (figures 3 and 4).

The inside of the scalp. The vessels are treated with heparin.
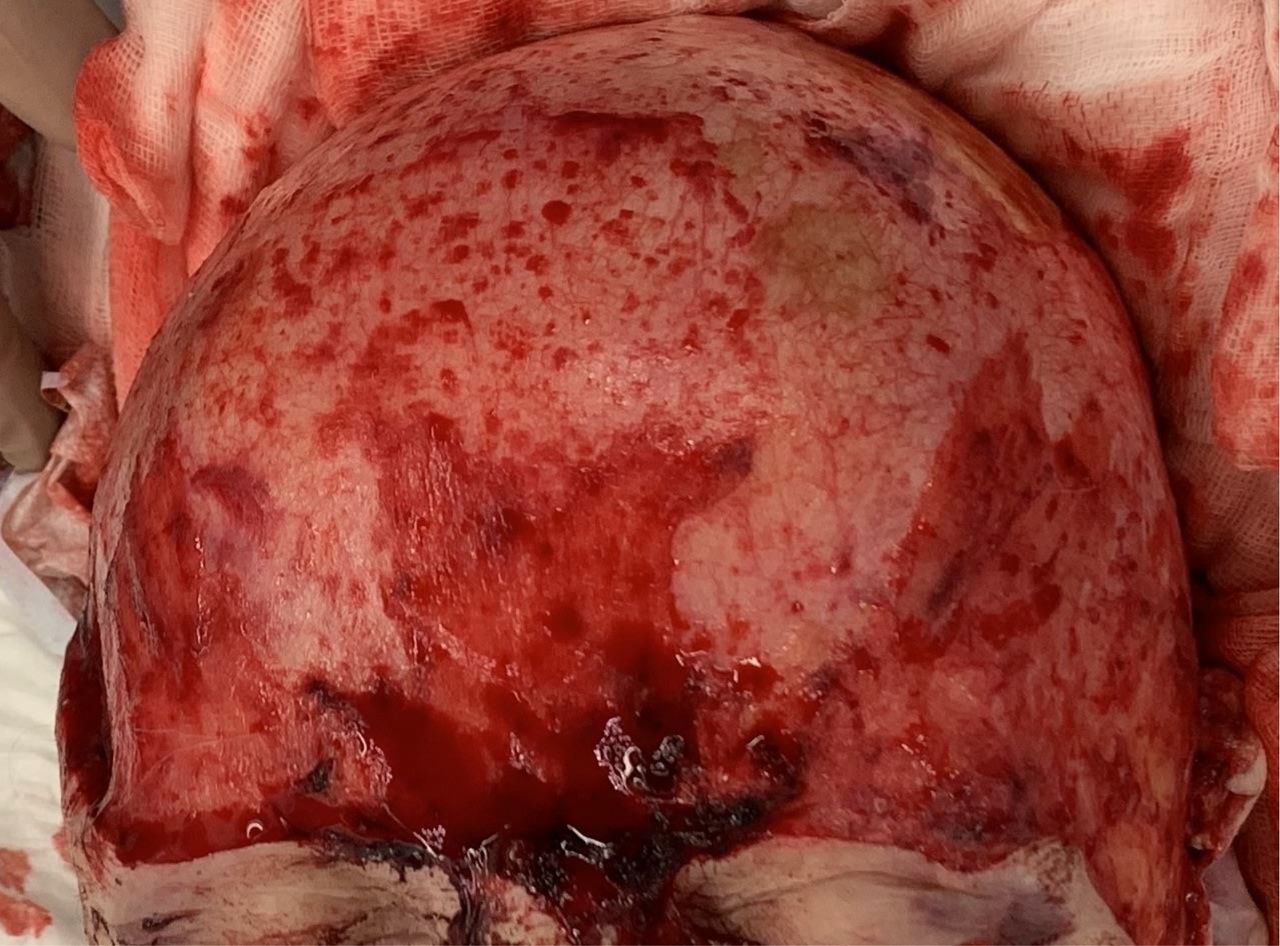
Frontal view of the patient’s head in the OR. OR, operating room.
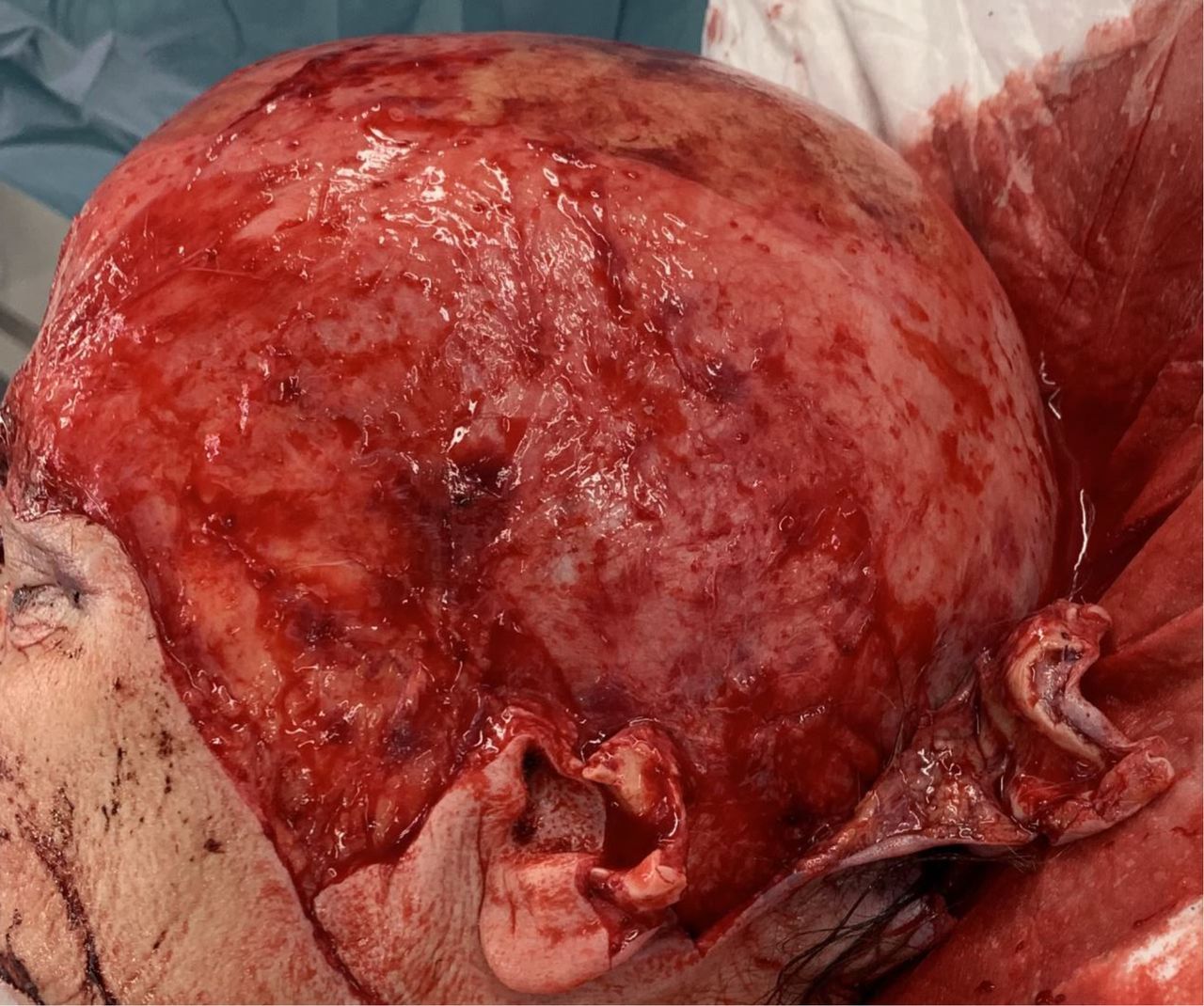
Side view of the patient’s head in the OR. OR, operating room.
The left superficial temporal artery was anastomosed using an Ethilon 10–0 suture (figure 5). The temporal vein on the left side was anastomosed using a 1.5 mm 3 M clip. Initially, the scalp was not perfused, probably because of hypothermia, but within 15 min the scalp was sufficiently perfused, which was demonstrated by good blood flow through the right temporal vein which was open. The right temporal vein was also anastomosed using a 1.5 mm 3 M clip. After 30 min of observation, the left vein showed signs of venous congestion such as rapid capillary refill time and a dark blue colour, which could be observed on the left side of the scalp. The anastomosis was cut and reanastomosed resulting in sufficient drainage of the scalp flap.

The left superficial temporal artery is marked with a suture.
Three drains were placed, one above the nose and one in each temporal region. The scalp was attached with surgical clips and 4–0 Ethilon suture. The upper cutaneous part of the ear was sutured with 4–0 nylon.
The patient and staff were instructed to keep the patient’s head elevated as much as possible and to only support the neck when needing assistance with mobilisation.
Outcome and follow-up
The patient had a very successful recovery, with no pain postoperatively. The flap was well vascularised and without any signs of necrosis or infection. The patient had partial necrosis of her left ear. She was discharged from hospital 5 days postoperatively (figure 6).

Five days postoperatively. Ready to be discharged.
The patient was seen 12 days postoperatively where she had her sutures and surgical clips removed (figure 7).

Twelve days postoperatively.
She was seen after 6 months where her hair was growing back nicely. She had no signs of alopecia, which is a relatively normal sequalae after a total scalp avulsion. Furthermore, she was regaining sensation in her scalp, and she had regained partial function of her frontalis muscle allowing her to lift her eyebrows (figure 8). She said that she was feeling progress week by week and she was very positive about the advancement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Six months postoperatively. The patient is regaining function of the frontalis muscle.
Discussion
A total scalp avulsion is a rare injury. It is most frequently women who suffer this kind of trauma because it is often a result of the entrapment of long hair in high-speed rotating industrial machinery.6
The first case of a scalp avulsion was described by Horovitz. In their case, the avulsed scalp was simply sutured back on without any microvascular anastomosis.7 The first successful replantation using microvascular anastomosis was described by Miller et al.8
The traumatic avulsion of a scalp will often result in haemorrhage. Singh et al described a blood loss of approximately 400 mL, which is similar to our case.1 The blood loss was not severe enough for the patient to need transfusion. In our case, the level of avulsion was loose areolar tissue which is similar to the case presented by Singh et al.1
Due to the low frequency of total scalp avulsions, no official consensus on treatment exists. However, Wechselberger et al have suggested an algorithm for treatment of total scalp avulsions.6
They suggest that replantation surgery should be used if possible. We agree that reimplantation surgery should always be applied if possible even in difficult cases such as an avulsed finger or in this case an avulsed scalp.9
The earliest articles describing microsurgical replantation of an avulsed scalp report a high number of anastomoses. Miller et al used five veins and both superficial temporal arteries.8 10 More recent literature has described quite a few total scalp avulsions that were sufficiently reimplanted using only one artery and one or two veins for microvascular reconstruction.6 11 This is in accordance with our experience. In our case, we performed one arterial anastomosis and two venous anastomoses.
After a review of the existing literature, we believe that this is one of the largest scalp avulsions to be replanted successfully. The large size of our scalp contributes to the existing consensus that one artery and two veins is adequate for sufficient blood supply for an entire scalp. During the microsurgical replantation of the scalp, we did not facilitate any interventions to enhance nerve regeneration. Despite our lack of intervention, the patient was slowly regaining neurological function of her scalp 6 months after replantation. The ability to regain sensation after the replantation of an avulsed scalp has previously been reported to approximately 6 months postoperatively, which is in accordance with our experience from this case.12 In future cases, neurological function should not necessarily be expected and is very difficult to evaluate perioperatively. However, some cases report that neurological function can return.
One should not expect the return of neurological function within the first 6 months after surgery.
Patient’s perspective
Written 5 months postoperatively.
I was very satisfied with the entire experience and very thankful for all the healthcare professionals that helped me from the trauma occurred until I was discharged from hospital.
I believe that the magnitude of the trauma combined with the fact that I only experienced a minimal amount of pain made it very surreal for me. I believe it was more traumatising for the people around me and my husband would agree. He told me that it was almost impossible to comprehend that a total scalp avulsion could be relatively pain free.
I am very delighted that I am not suffering from alopecia, which I have been told is a well-known problem after a scalp avulsion. My hair is slowly growing back which is helping me achieve the same appearance that I had prior to my accident. My hair covers the defect on my left ear completely. Furthermore, I am starting to regain sensation in my scalp. It is slowly getting better week by week. This continues progress gives me a lot of faith for the future.
Learning points
When presented with a scalp avulsion we recommend the following line of thought.
First, you need to assess if the scalp avulsion is the sole injury or if there are other injuries that need taking care of. Due to the magnitude of the trauma and the rarity of the case, it is easy to focus all your thoughts on the potentially challenging scalp replantation. We did a CT of the cerebrum, facial bones and cervical spine to rule out intracranial haemorrhage and fractures. This allowed us to focus all our energy on the replantation once the other potential injuries were ruled out.
Second, the scalp flap should be examined. Is it well preserved? What is the cold and warm ischaemia time, respectively? Is there a loss of substance (ie, is the scalp flap large enough for a sufficient coverage of the cranium)? If not, what options do we have in terms of skin grafting, local flaps or free flaps?
Third, how many and which afferent and efferent vessels are available for anastomosis? Are these vessels reliable for sufficient blood supply and drainage?
Fourth, how to attach the scalp after micro anastomosis: We used surgical clips combined with 4–0 nylon sutures. Furthermore, we placed a drain above the nose and one in each temporal region for sufficient drainage.
Fifth, how to monitor the scalp: colour, temperature, capillary response, Doppler, microdialysis? These variables can vary from department to department. It is vital to monitor the scalp closely and to have a continuous dialogue with senior colleagues.
Ethics statements
Patient consent for publication
Footnotes
Contributors CBM, LP, VB and JAS: planning, conduct, reporting, design, acquisition of data, proof reading. LP and VB were the doctors called to the trauma center for an initial examination. In the OR, all four authors were present and participated in the replantation surgery. All four authors have contributed with written passages of the article, LP and VB with the prehospital information and initial examination. JAS with the replantation details and follow-up. All four authors have contributed with proof reading of the article and have made significant contributions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.