Article Text

Abstract
Hearing loss following COVID-19 infection has been scarcely reported in the literature.
A previously well middle-aged man presented to the emergency department with breathlessness and cough 8 days after testing positive for COVID-19 in the community. The patient was treated in the intensive care unit due to respiratory failure. Following extubation and step down to ward-level care 2 months later, the patient reported sudden left-sided hearing loss and tinnitus. Ear examination was unremarkable and pure tone audiometry revealed profound left sensorineural hearing loss. MRI of the internal acoustic meatus did not show any cerebellopontine lesions. Intravenous steroid therapy as well as oral steroids were not successful in improvement of hearing.
A few cases of COVID-19-associated sensorineural hearing loss have been reported; the majority report irreversible loss. Awareness of this phenomenon and early referral for specialist review and audiological assessment to attempt salvage of hearing can reduce hearing disability.
- Ear, nose and throat/otolaryngology
- Public health
- Otolaryngology / ENT
Statistics from Altmetric.com
Background
Since the declaration of the COVID-19 pandemic, infection with the disease has presented with a myriad of symptoms affecting almost all systems of the human body, not only limited to the respiratory tract.1 Research on the pathophysiological processes of the virus supports the premise that COVID-19 can affect all organs.2 Adverse neurological manifestations of COVID-19 infection have been well documented and can manifest in isolation or in combination with the typical respiratory symptoms.3 Associated symptoms, such as headaches, dizziness, anosmia, rhinorhoea, nasal congestion, taste disturbance and swallowing dysfunction, are of particular interest to otolaryngology specialists. Many patients seek referral to outpatient otolaryngology services due to a protracted course, or a failure in resolution of the aforementioned symptoms. Although a prolonged course of symptoms affecting the upper aerodigestive tract post-COVID-19 infection are not uncommon (‘long COVID19’ is an established entity), there have been few reported cases affecting hearing following COVID-19 infection. Of the sparse number of cases reported of COVID-19-related unilateral hearing loss, the majority of accounts report an irreversible loss.4 5 Attempts to explain this phenomenon propose that excess cytokine release in the hearing centre of the medulla oblongata during COVID-19 infection causes increasing amounts of oxidative damage and thus, permanent hearing loss.6 Further to this, as COVID-19 infection is a recognised precursor for hypercoagulability, microthrombi or emboli within small vessels supplying the hearing centre have been hypothesised to cause a degree of ischaemic injury.6 A recent systematic review of existing literature concluded that hearing loss, dizziness and tinnitus were statistically significant symptoms in patients with COVID-19 infection.7
Raising awareness of the potential of COVID-19 infection to cause permanent hearing loss is important for primary care doctors as well as otolaryngology specialists. Similar presentations as described in this communication ought to encourage general practitioners to promptly commence oral steroid therapy as an attempt to salvage hearing as well as early referral for audiological assessment and otolaryngology review. Earlier treatment with steroid therapy has been shown in some cases to improve sudden sensorineural hearing loss.8 9 Failing this, timely referral for hearing aid devices has the benefit to improve patients’ quality of life following complete hearing loss as well as reduce the impact of hearing disability.
Case presentation
A man in his early 50s was admitted to hospital with worsening shortness of breath and cough 8 days after testing positive for COVID-19 in the community. The patient was normally fit and well with no significant medical history, regular medications or known drug allergies. The patient worked in construction and denied a history of exposure to loud noises or head trauma.
The patient was admitted and treated for COVID-19 pneumonitis, with management comprising continuous positive airway pressure (CPAP) as well as oxygen therapy on the intensive care unit (ICU), intravenous steroids, intravenous antivirals, Pabrinex and ascorbic acid. During the initial peak of the COVID-19 pandemic, this treatment was administered as standard medication to patients admitted with COVID-19 pneumonitis within the admitting district general hospital (also known as the ‘COVID-19 bundle). Following initial intravenous steroid therapy, a reducing course of oral prednisolone was continued for 1 month in ICU.
Respiratory support was escalated to invasive ventilation following a lack of improvement on CPAP. The patient remained as an inpatient in the ICU for approximately 2 months and received positive pressure ventilation for the duration of this time.
On step down to the medical ward, the patient reported sudden-onset complete left-sided hearing loss and described an intermittent ‘high pitched ringing sensation in the left ear’ which was not pulsatile in nature. The patient presumed these symptoms to have commenced a week prior to step down to ward-level care. There were no associated symptoms of otalgia, otorrhoea, vertigo or aural fullness bilaterally, nor were there any complaints of hearing loss of the right side.
On examination, both ear canals were unremarkable in appearance and tympanic membranes were intact bilaterally. There were no signs or symptoms of mastoid disease.
The patient was commenced on a week’s course of oral prednisolone 40 mg 7 days after the initial report of unilateral sudden-onset hearing loss.
Although the patient received high-dose intravenous steroids during initial admission for the COVID-19 infection, a tapering course of oral steroids for a month following this, as well as further oral steroids 1 week following report of the unilateral hearing loss, there was no reported improvement of left-sided hearing following these treatments at discharge, or at 1-year follow-up.
Investigations
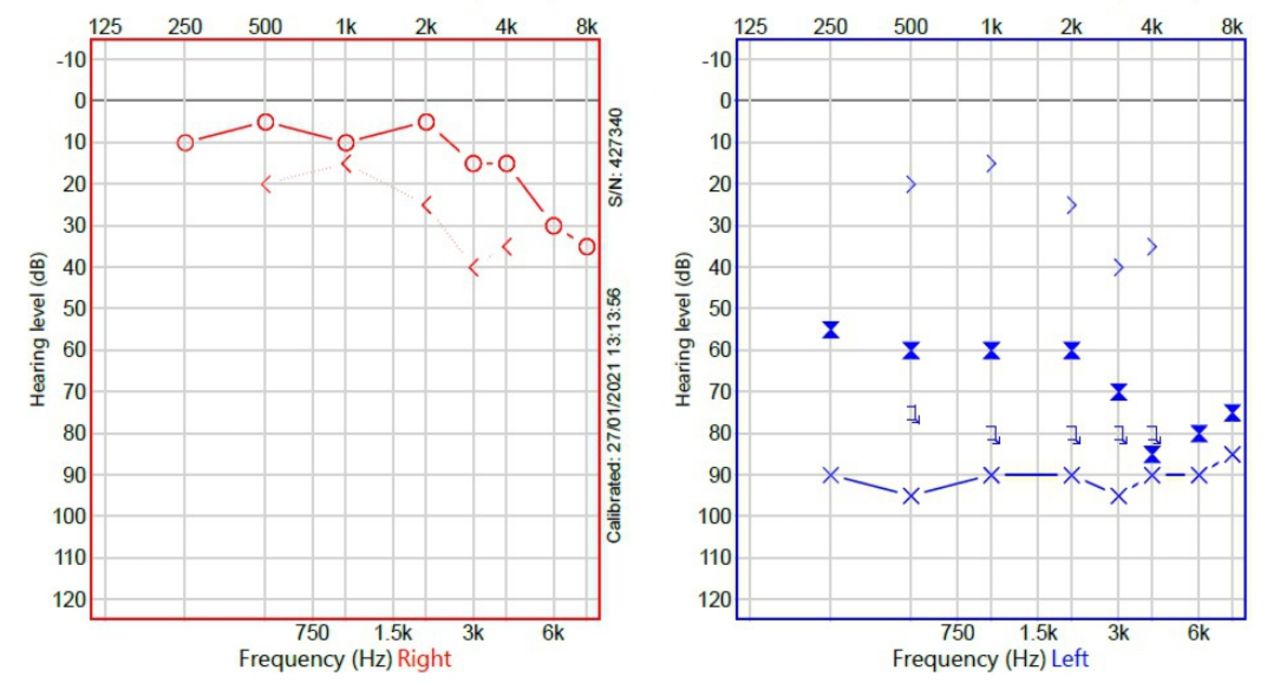
Pure tone audiometry showed a profound unilateral sensorineural left-sided hearing loss across all frequencies, as shown in figure 1. Tympanometry revealed type As tympanograms bilaterally.

{kind=link}
Audiogram to show left-sided profound hearing loss across all frequencies.
MRI of the head and internal acoustic meatus’ revealed no overt abnormalities, with normal appearances of the inner ear structures and satisfactory appearances of the brain parenchyma and cerebral spinal fluid spaces. This scan also concluded that there were no focal lesions at the cerebello-pontine (CP) angles or within the internal auditory canals.
Differential diagnosis
There are important differential diagnoses to consider with a presentation of unilateral sudden-onset hearing loss. An idiopathic sudden-onset sensorineural hearing loss can be considered as a cause for the symptoms experienced in this case and would be the leading differential diagnosis, especially when taking into account that there have been few reported incidences of COVID-19-related sensorineural hearing loss in the existing literature. Despite this, there have been accounts of viral-induced sensorineural hearing loss described.10
Other chief pathologies to consider in this case is a potential vestibular schwannoma which could account for the symptoms of unilateral sensorineural hearing loss. This often presents as gradually worsening hearing, however, it is not uncommon for such lesions to present with sudden-onset hearing loss.11 MRI of the internal auditory acoustic meatus’ confirmed there were no CP angle lesions visible and thus this diagnosis was reliably excluded.
Another critical cause to consider in a patient presenting with sudden-onset sensironeural hearing loss is a possible cerebrovascular accident affecting the posterior circulation of the brain. This was deemed unlikely on history and clinical examination of the patient and moreover, MRI of the brain did not support this diagnosis.
Common conductive causes of hearing loss such as infection of the outer ear canal, middle ear or cerumen impaction were excluded by an unremarkable examination of the ears. Furthermore, there were no reports of otalgia, otorrhea or associated ear symptoms from the patient.
Treatment
The patient was admitted to the ICU due to respiratory failure secondary to COVID-19 pneumonitis. Following a failure to maintain optimal oxygen saturations with the utilisation of CPAP ventilation, the patient was escalated to invasive ventilation. Initial treatment consisted of 6 mg of intravenous dexamethasone for three stat doses and supplemental vitamins) in the form of Pabrinex (vitamin B supplements), ascorbic acid (vitamin C supplements) and intravenous remdesivir (antiviral): the ‘COVID-19 bundle’ which was administered to all patient admitted to hospital with COVID-19 pneumonitis, provided there were no overt contraindications. A reducing course of oral prednisolone was continued for 1 month in ICU following initial intravenous steroid therapy.
Following step down to the medical ward approximately 2 months following ICU admission, 40 mg of oral prednisolone was started for 7 days: this was 1 week after the reported initial onset of unilateral hearing loss and tinnitus.
The patient did not receive any ototoxic medications throughout the duration of inpatient stay.
Outcome and follow-up
The patient was discharged after a total of 3 months in hospital following a progressive recovery from COVID-19 infection and improvement of chest symptoms.
Prior to discharge from the hospital, and despite various courses of intravenous and oral steroid therapy while an inpatient, there was no reported improvement of hearing of the left ear.
Furthermore, at follow-up with the otolaryngology team 3 months following discharge from hospital, there was no report of return of hearing to the left side. The patient was subsequently referred to audiology services for a contralateral routing of signals hearing aid and hearing rehabilitation for the unresolved left sided unilateral sensorineural hearing loss. At 1-year follow-up, the patient did not experience any spontaneous improvement of the complete left-sided hearing loss.
Discussion
Ongoing research into the short-term and long-term effects of the COVID-19 virus has yielded an abundance of emerging literature surrounding the physiological effects of the virus on the human body. Although symptoms and pathology of the upper aerodigestive tract has been well-recognised post-COVID-19 infection, there is little literature pertaining to the possible effects of COVID-19 on the ears and, specifically, hearing loss.
Sudden-onset sensorineural hearing loss is an important entity and timely management is important to prevent hearing disability. It is reported that sensorineural hearing loss is an uncommon complication following viral infections, and even less following COVID-19 infection.10
Although uncommon, sensorineural hearing loss following viral infection has been described in the literature, proposing that various viral infections can affect hearing, with mechanisms of hearing loss presumed to result from direct damage to important inner ear structures such as the organ of Corti and inner hair cells.12 Further to this, recent accounts describe both unilateral and bilateral sensorineural hearing loss noted in patients post-COVID-19 infection.13
In this particular case report, there was a lack of improvement in the patients’ hearing despite various courses of intravenous and oral steroid therapy as an inpatient. Similar outcomes have been previously reported in COVID-19 positive patients with unresolving sensorineural hearing loss, despite attempts at salvage steroid therapy.4
Theories speculate that COVID-19 formally known as SARS-CoV-2 attaches to β-chain haemoglobin within red blood cells and infects body tissues by binding to ACE-2.13 This complex subsequently activates cytokine release. As ACE-2 is abundantly present within medulla oblongata and temporal lobe of the brain, damage to the these areas which house vital structures such as important sensory pathways as well as the hearing centre, can lead to hearing loss. Moreover, hypoxia caused by SARS-CoV-2 can further damage the hearing centre.13 Novel research has further hypothesised that a relapsing demyelinating disease process within the brainstem can lead to auditory involvement and damage.14
It must be noted in this case that the failure of timely commencement of oral steroid therapy in hopes to salvage the patients’ hearing could, in effect, have contributed to a failure of recovery. This is because the complaint of hearing loss was formally reported shortly after the patient was transferred to the medical ward, after an intial 2-month inpatient stay in ICU for invasive ventilation. In theory, the patients’ hearing loss could have occurred at any point during the 2 months in ICU, however, this would not have been reported until the patient was able to verbally communicate the loss of hearing. Although early intravenous steroid therapy followed by a tapering course of oral steroids were administered in ICU for the purpose of treating COVID-19 pneumonitis, it remains unclear at which point the hearing loss truly commenced.
There is still little understanding of the relationship between COVID-19 infection and hearing loss. It has been postulated is that the cytokine storm following COVID-19 infection can lead to a thrombosis and hyperinflammation of the endothelium,15 with postmortem reports of COVID-19 positive patients showing that endothelial inflammation and microvascular thrombosis is prominent in small vessels of certain organs.16 These concepts provide plausibility to the theory that compromise to the blood supply of the vestibulocochlear nerve can be implicated as a cause for sensorineural hearing loss following infection with COVID-19 virus.
Interestingly, comparing amplitudes of transient evoked otoacoustic emissions (TEOAE) and pure tone audiometry thresholds in asymptomatic COVID-19 positive patients vs patients without infection showed that COVID-19 positive patients had significantly worse amplitude of TEOAE as well as higher pure tone audiometry frequency thresholds.17 Such evidence suggests that the affects of COVID-19 infection can potentially damage cochlear hair cells even in asymptomatic patients.
This case highlights the importance of early investigation and appropriate management in order to reduce hearing disability and thus quality of life in patients that present with hearing loss post-COVID-19 infection. An increased global awareness of this phenomenon, prompt recognition by primary care physicians as well as secondary care doctors with timely referral to otolaryngology and audiology services predicts a reduction of hearing disability as a result.
Although the existing literature is sparse pertaining to a causal relationship between severe COVID-19 infection and sensorineural hearing loss, the majority of accounts report irreversible hearing loss.5 Authors also urge that it must be acknowledged that throughout the course of the pandemic, certain medications used have been found in the literature to cause ototoxicity and/or hearing loss, such agents include azithromycin, hydroxychloroquine and chloroquine.18 19 These findings must be recognised and considered prior to drawing inferences regarding COVID-19-induced hearing loss in future explorations. Future cases ought to provide further evaluation of the success of steroid therapy in probable COVID-19-induced sudden sensorineural hearing loss.
Patient’s perspective
My experiences during this time were initially very satisfactory. Since admission to the Intensive Care Unit (ICU) with severe COVID-19 pneumonitis, the only reason I am still here to report about this is due to the exemplary work done by the staff in intensive care to keep me alive.
However, since being discharged from the hospital, my patient after-care and follow-up has been poor to mostly non-existent. I have had to chase every follow-up including referral to ear, nose and throat for hearing loss. It was frustrating to be told I was ‘out of area’.
At the time my wife was also critically ill in hospital in a ward bed across from my own; she had all procedural follow-ups within a 4–6 week period after discharge.
It has been 18 months since my initial diagnosis and I am waiting follow-up imaging for my lungs, especially as am known to have chronic obstructive pulmonary disease (COPD).
I had many difficulties and a delayed referral to the ENT department due to being ‘out of area’ of the hospital I was initially treated in.
I am still suffering with many symptoms and problems post-COVID and am still awaiting further assessments to determine the extent of damage caused by COVID-19 to my body.
Learning points
COVID-19-related unilateral hearing loss is a recognised phenomenon of which primary care doctors, secondary care specialists as well as the wider patient population ought to be aware of.
Current accounts in the literature report an irreversible loss of hearing following severe COVID-19 infection.
Future cases should aim to determine the success of steroid therapy in treating COVID-induced sudden sensorineural hearing loss.
Prompt recognition and referral for audiological assessment and otolaryngology specialist review predicts a more hopeful prognosis and should comprise attempting salvage steroid therapy and/or offering hearing devices early to reduce hearing disability.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors SA, DG and WJL contributed equally to the clinical care, communications with the patient as well as the write-up of this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.