Article Text

Statistics from Altmetric.com
Description
A woman in the 70s presented with fever, leg oedema and gait instability for 3 weeks. She had no headache, respiratory symptoms, gastrointestinal symptoms, dysuria, arthralgia or skin rash. She was alert, and her vital signs were normal except for a body temperature of 37.8°C. Physical examination revealed splenomegaly, generalised pitting oedema and gait instability; neurological examination was normal except for gait instability. Laboratory testing revealed anaemia (haemoglobin, 88 g/L), thrombocytopaenia (platelet count, 92x109/L) and liver dysfunction (aspartate aminotransferase, 51 U/L; alanine aminotransferase, 36 U/L; lactate dehydrogenase, 716 IU/L; total bilirubin, 0.4 mg/dL). Her serum soluble interleukin-2 receptor and ferritin levels were high at 12 800 U/mL and 3121 ng/mL, respectively. Non-contrast-enhanced CT revealed mild splenomegaly. The blood and urine cultures were normal. Bone marrow examination demonstrated hypocellularity, haemophagocytosis and the presence of large abnormal lymphoid cells. However, there was no evidence of an abnormal cell population on flow cytometry of the bone marrow. Brain MRI performed to determine the cause of the fever and unexplained gait instability revealed a hyperintense lesion in the central pons on T2-weighted imaging, diffusion-weighted imaging and fluid-attenuated inversion recovery imaging (figure 1A, white arrow indicating the lesion). Cerebrospinal fluid cytology and culture revealed no abnormality. Random skin biopsies revealed atypical lymphocytes within the small vessels of the dermis and hypodermis (figure 2A). The immunophenotype of these cells was consistent with B-cell phenotype, showing CD20 and CD79a (figure 2B). Accordingly, intravascular large B-cell lymphoma (IVLBCL) was diagnosed. She was treated with R-THP-COP (rituximab, tetrahydropyranyl adriamycin, cyclophosphamide, vincristine and prednisolone) for eight cycles. Hyperintense lesion in the pons was almost undetectable on MRI after 5 months of chemotherapy (figure 1B), and complete remission was achieved after eight cycles of chemotherapy.
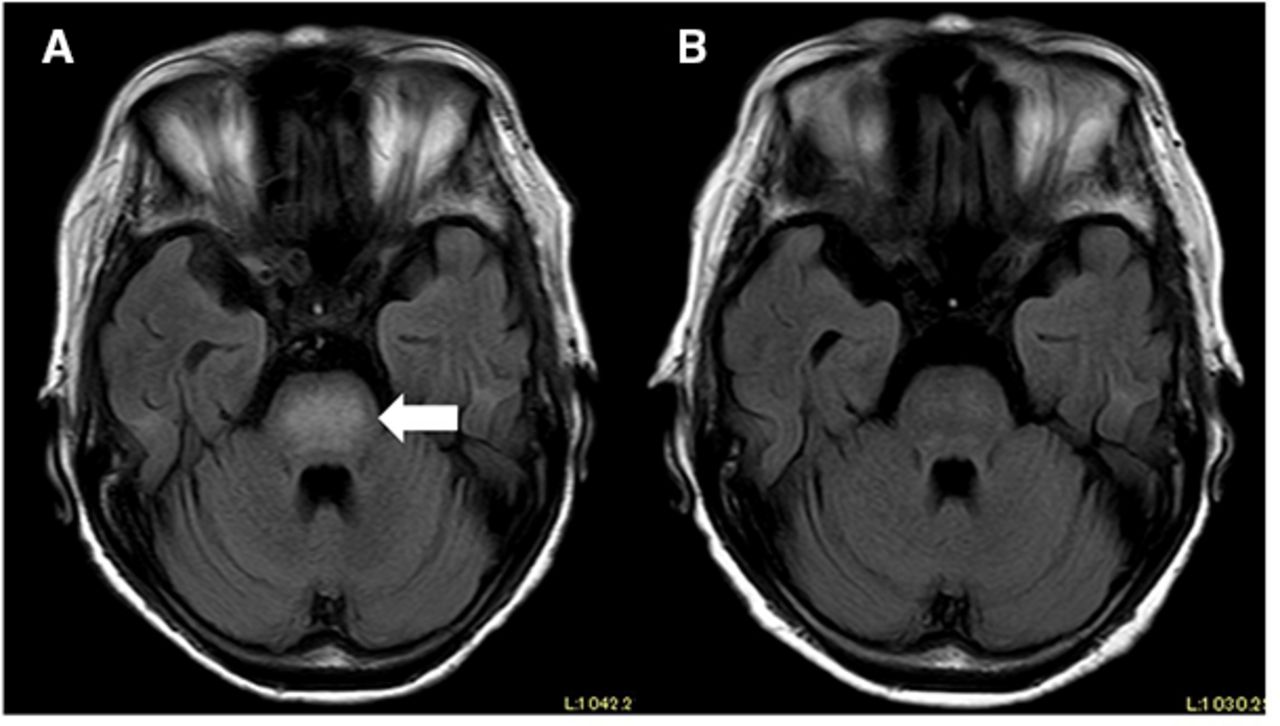
Brain MRI shows a hyperintense lesion in the central pons (white arrow) on fluid-attenuated inversion recovery images (A) that was almost undetectable after 5 months of chemotherapy (B).

{kind=link}
{kind=link}
H&E staining of skin biopsy shows exhibited large, scattered abnormal cells clustered in the small vessels (A). Immunohistochemical staining of skin biopsy shows CD20-positive cells within the small vessels (B).
IVLBCL manifests abnormal MRI findings in approximately 90% of patients.1 High-intensity lesions in the pons, which are found in about 60% of patients, have been reported to exhibit potential diagnostic value, because this MRI finding has rarely been reported in other pyrogenic diseases or other subtypes of lymphoma.1 Generally, in pontine lesions, multiple neurological signs are observed: impaired consciousness (ascending reticular activating system), weakness (corticospinal tract causes and facial nerve), dysarthria and dysphagia (corticobulbar tract), lateral gaze (abducens nerve and medial longitudinal fasciculus), facial sensation (trigeminal nerve) and ataxia (cerebellar peduncle). However, it has been reported that approximately half of the patients who showed these imaging findings were asymptomatic; hence, these imaging changes in lymphoma patients may not be consistent with their symptoms. The most important differential diagnosis for this imaging finding is osmotic demyelination syndrome, which can be excluded in this case because there was no rapid correction of hyponatraemia. Pons infarction and other central demyelinating diseases are also differential diagnoses, but these are less likely to be associated with thrombocytopaenia and splenomegaly.
In patients with undiagnosed fever with neurological symptoms, the presence of this specific MRI finding may contribute to reduce the time to diagnose IVLBCL, thereby providing a positive impact on the early initiation of treatment and improving prognosis.
Learning points
Intravascular large B-cell lymphoma manifests abnormal MRI findings in approximately 90% of patients, and high-intensity lesions in the pons, which are found in about 60% of patients.
Osmotic demyelination syndrome, pons infarction and other central demyelinating diseases are also differential diagnoses, but these are less likely to be associated with thrombocytopaenia and splenomegaly.
Ethics statements
Patient consent for publication
Footnotes
Contributors KK and YI identified significance. KK wrote the manuscript, TT and TS revised it. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.