Article Text

Abstract
We present a rare case of destructive osteomyelitis of the sternum caused by Parvimonas micra and Campylobacter rectus. A previously healthy female patient in her 40s presented to the emergency department due to a spontaneous rupture of an abscess located to the chest wall. Imaging confirmed abscess formation with osteomyelitis of the sternum. Emergent surgical debridement was performed, blood and bone cultures were taken and the patient received antibiotic treatment. Cultures of the bone and deep tissue revealed infection with Parvimonas micra and Campylobacter rectus, both being members of the oral flora and associated with chronic periodontitis. Receiving targeted antibiotic treatment, our patient made a quick recovery. After treatment of the osteomyelitis, our patient was referred to the dentist where chronic periodontitis could be confirmed. Invasive infections with Parvimonas micra and Campylobacter rectus are rare. Investigation of a dental origin is crucial to prevent recurrent infections.
- Bone and joint infections
- Dentistry and oral medicine
- Emergency medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Primary osteomyelitis of the sternum is a rare disease, accounting only 0.3% of osteomyelitis case reports. While secondary osteomyelitis of the sternum is most commonly seen as a complication after a surgical intervention or trauma, primary osteomyelitis of the sternum occurs secondary to bacteraemia. Intravenous drug abuse, diabetes mellitus or immune deficiency are known predisposing factors.1 2 Most commonly, primary osteomyelitis is caused by a single pathogen, and Staphylococcus aureus and Pseudomonas aeruginosa being the most common pathogens.3 4 Only a limited number of case reports have reported about particular osteomyelitis due to Parvimonas micra, for example, in the distal phalanx of the thumb5 or hip joint,6 but no article has been found about osteomyelitis of the sternum caused by P. micra or Campylobacter rectus.
P. micra are anaerobic, gram-positive cocci, formerly described as Peptostreptococcus micros and Micromonas micros.7 P. micra has been associated with meningitis,8 cervical and brain abscess,9 10 spondylodiscitis11 as well as endocarditis12 and native joint infections.13 In 2018, van Duijvenbode et al performed a systematic review where four cases of spondylitis and nine cases of spondylodiscitis were identified.14
C. rectus is also a member of the oral flora.15 An investigation of selected bacterial species in endoperiodontal lesions, performed in 2012 by Didilescou et al, revealed extremely high bacterial loads in endodontic samples for P. micra together with C. rectus.16 17 C. rectus is a straight, non-spore forming and motile gram-negative rod, which has first been described in 1981 as Wolinella recta.15 In 1991, the organism was transferred to the genus Campylobacter based on phylogenetic studies.18 Invasive infections with C. rectus have rarely been reported in the literature, and to our knowledge, only one case of clival osteomyelitis has been noted so far.19 One fatal case of thoracic empyema involving C. rectus is reported.20 Although little is known in regard to pathogenic potential of C. rectus, dental caries, periodontitis, poor oral hygiene or malignancies have been identified as predisposing factors of invasive C. rectus infections.18 21
To our knowledge, no similar case report of osteomyelitis of the sternum caused by P. micra or C. rectus has been described in literature before. Therefore, we hereby present a rare case of destructive osteomyelitis of the sternum caused by P. micra and C. rectus infection; both are members of the oral flora and associated with chronic periodontitis.
Case presentation
A female patient in her mid-40s presented to the emergency department (ED) of a regional hospital in Switzerland due to a spontaneous rupture of an abscess located on the mid-frontal chest wall. The patient was of Tanzanian origin and had lived in Switzerland for the past 30 years. Medical history was unremarkable. The patient did not take any medication. Due to good health, the patient rarely visited her general practitioner. No regular check-ups were performed in the last decade.
Detail history taking revealed that the patient had noticed a progressive swelling of the chest wall over the past 4 weeks. Furthermore, the patient experienced some general discomfort and loss of appetite. She did not notice any fever, and the pain was bearable without taking any painkillers or had the need to seek medical help. At the day of presentation, the abscess ruptured spontaneously with discharge of a remarkable amount of pus, which is why the patient visited the ED.
At the time of ED presentation, the patient had no fever (36.3°C). The blood pressure was within the normal range (137/92 mm Hg), but mild tachycardia was noted (113 beats per minute). Physical examination revealed a significant swelling of 20×10 cm on the chest wall reaching from the processus xyphoideus up to the upper border of the sternum. Under the left clavicle, the abscess had perforated the skin with discharge of bad-smelling purulent fluid and blood (figure 1). The remaining examination was unremarkable. There were no signs of intravenous drug abuse. No entry point of infection could be determined on physical examination.

Patient on emergency department presentation.
Investigations
Laboratory testing showed elevated C reactive protein (CRP) levels (402 mg/L, normal range <10 mg/L), elevated white cell count (15.4 G/L; normal range 4.5–10.5 G/L), elevated thrombocyte count (429 G/L; normal range 150–350 G/L) and slightly elevated serum creatinine (102 µmol/L; normal range 46–92 µmol/L). Measured procalcitonin also was significantly elevated (44 µg/L; normal range <0.1 µg/L).
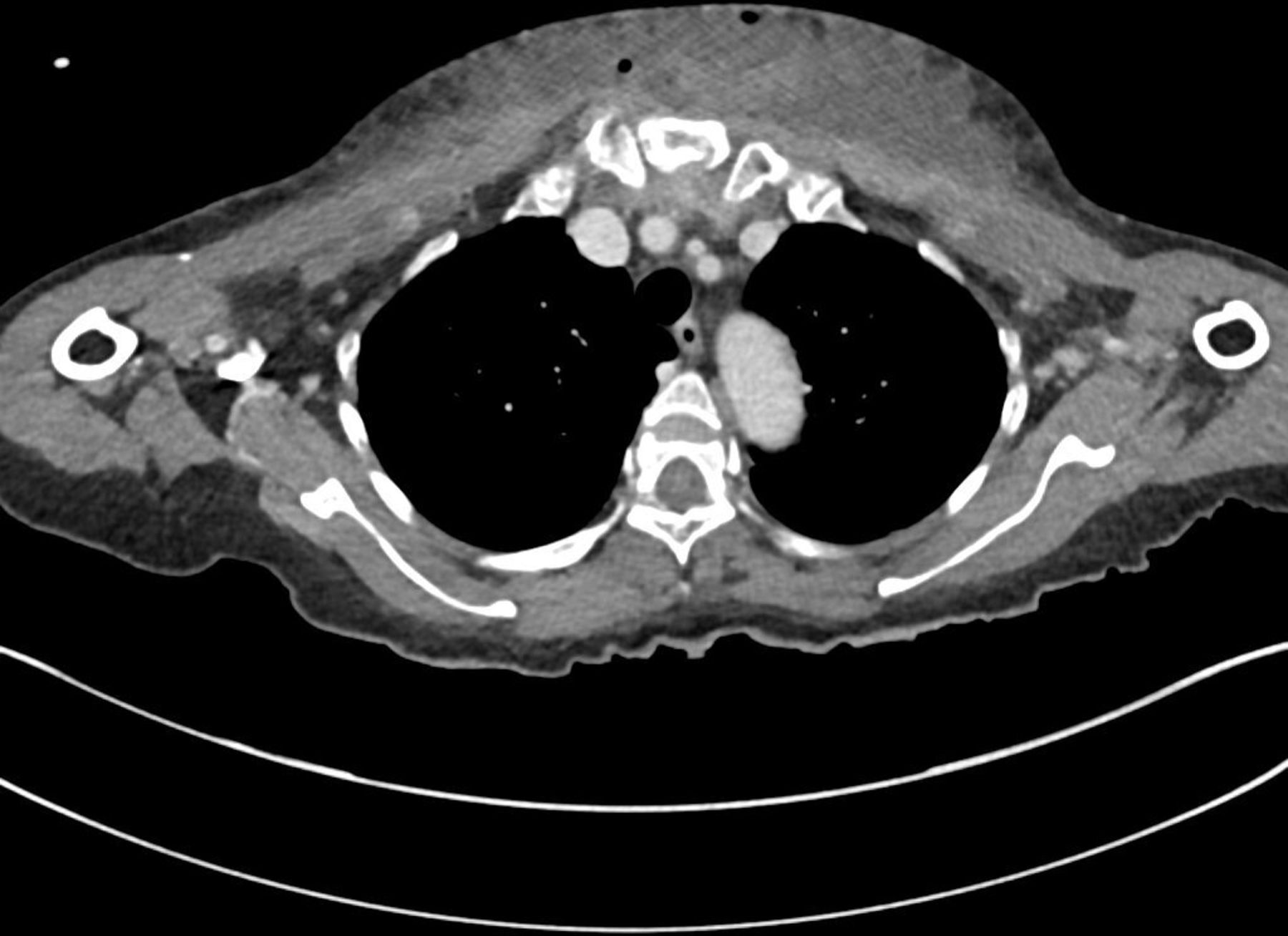
CT was performed to assess the extent of the abscess formation of the chest wall (figures 2 and 3). Imaging revealed osteomyelitic erosion of the sternum with abscess formation reaching from the processus xyphoideus of the sternum up to the left side of the glandula thyreoidea, compromising the sternoicleidomastoid muscle. The abscess measured 20×13.5 cm. No abscess formation was seen in the intrathoracic or mediastinal space.

CT scan of the abscess at the level of the neck.

CT scan of the abscess at the level of the sternoclavicular joint.
Cultures of the blood were asserted, and the patient was referred to prompt surgical debridement where diagnostic investigation was completed by taking deep tissue and blood samples for microbiological assessment. In cultures taken from the sternal bone tissue and deep tissue, P. micra and C. rectus were isolated. There were no antimicrobial resistances reported neither to P. micra nor to C. rectus. Mycobacterial cultures were negative.
Since P. micra and C. rectus are both members of the oral flora, a dental origin of infection was considered. The patient reported to not have seen a dentist for more than 10 years, while dental hygiene seemed rather poor. Our patient therefore was referred to the dental department where a chronic periodontitis was diagnosed. Tooth 47 was not vital, and loss of previous cavity occlusion was reported in tooth 36. Remaining dental examination remained unremarkable.
In conclusion, the patient was diagnosed with primary osteomyelitis of the sternum with abscess formation most likely due to chronic periodontitis.
Differential diagnosis
Primary osteomyelitis of the sternum is rare. In literature intravenous drug abuse, diabetes mellitus or immune deficiency is described as predisposing factors. However, our patient appeared to be previously healthy. Anamnesis and clinical examination did not reveal any indication of intravenous drug abuse. HbA1c was normal, underlying diabetes mellitus could be therefore excluded. An underlying immunodeficiency such as HIV-infection could be excluded by serological testing, and our patient did not take any immunosuppressive medication.
The patient was of Tanzanian origin and had lived in Switzerland for more than 30 years. Her last visit to Tanzania dated back to 7 years. On presentation, an extrapulmonary manifestation of tuberculosis could not be excluded. However, cultures on mycobacterium tuberculosis as well as PCR testing were repeatedly negative.
A malignant cause of bone manifestation with secondary infection was considered; however, a primary tumour could not be detected on CT scans, and a gynaecological examination including Papanicolaou-test remained normal. The patient refused a gastroscopic and colonoscopic examination. The collected samples from the sternum did not show any malignancies, and due to good response on antibiotic treatment and detection of pathogenic bacteria, a malignant cause of the sternal lesion was considered highly unlikely.
In our case, detection of microorganisms belonging to the oral flora was the crucial factor in finding a dental entrance point. However, a thorough oral examination took place only after receiving the indicative microbiological test results.
Treatment
Emergent treatment with extensive surgical debridement was performed, and empiric antibiotic treatment was initiated with piperacillin/tazobactam after surgery. Already after 24 hours of treatment, CRP levels were decreasing notably, so antibiotic treatment was de-escalated to clindamycine and doxycycline. After blood and deep tissue cultures revealed infection with P. micra and C. rectus, antibiotic treatment was adjusted to co-amoxicillin. The patient furthermore underwent sequential surgical debridement with vacuum-assisted closure therapy and finally with split-skin grafting (figures 4 and 5).

Intraoperative image following surgical resection.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Four weeks postoperative following split-skin grafting.
Outcome and follow-up
The patient made a quick recovery with normalisation of blood parameters and well-healing wound of the chest wall. Four weeks after hospital admission, the patient was discharged to a rehabilitation centre and returned home 2 weeks later. On discharge, the patient did not need any further pain medication.
The patient was followed up in the outpatient clinic for infectious diseases . She reported a full recovery with no remaining complaints. Antibiotic therapy was planed to be continued for an overall period of 6 weeks according to the guidelines of antibiotic treatment of osteomyelitis.22 23 Due to a delay in follow-up visits, the antibiotic therapy was continued for an overall period of 8 weeks and thereafter could be stopped.
To prevent further infections, periodontitis treatment including plaque removal and surgical pocket removal was recommended by our in-house dentists. Furthermore, extraction of the non-vital tooth 47 was indicated just as restoration of the lost cavity occlusion restoration of tooth 36. The patient preferred to perform the dental procedures at her own dentist. Therefore, the patient finally was discharged to further follow-up appointments at her own general practitioner and dental treatment at her own dentist. During a consultation 6 months after discharge, patient reported good health with no remaining deficits.
Discussion
Invasive infections, especially osteomyelitis, with P. micra as well as C. rectus are rare.5 15 19 In our patient, diagnosis could be confirmed by growth in standard cultures of the sternum as well as in standard cultures from the surrounding tissue. However, the detection of P. micra as well as C. rectus in the standard media is difficult,24 but nevertheless, P. micra was identified in standard cultures.
In August 2020, a systematic literature review of P. micra in spondylodiscitis identified 16 cases.12 In 50% of all cases, a dental cause or preceding dental was reported.12 Another systematic review also published in August 2020 could show that P. micra bacteraemia was associated with spondylodiscitis, oropharyngeal infection, abdominal abscess and septic pulmonary emboli.25 However, sternal osteomyelitis was not reported.25
A systematic literature review published in July 2021 on invasive infections with C. rectus revealed 20 cases, and no case showed a sternal osteomyelitis.26 In 55% of all patients, dental health issues were documented as the aetiology of infections.26 Furthermore, in 2007, a large study performed in southern Finland detected C. rectus in 31.3% of healthy adults, supporting the theory of dental origin of infection with C. rectus.16
In our patient, the poor oral status was not documented at admission. In clinical practice, an oral focus may be missed, especially in the acute setting of the ED, where the primary focus lies on haemodynamic and respiratory stabilisation of the patient. Only after identification of P. micra or C. rectus, an oral focus was considered, which highlights the importance of pathogen identification to guide adequate treatment. It also shows how important it is, despite overcrowded ED, to perform a complete physical examination, including oral examination. This is also the only way to be sure not to miss an infectious focus, leaving us here to emphasise above all the importance and necessity of a complete physical examination.
Concerning treatment, P. micra is highly susceptible to antibiotics, and some studies showed only low rates of antimicrobial resistance.27 28 Murdoch et al found P. micra to be most susceptible to penicillin, followed by metronidazole and clindamycin.29 There is few literature on antibiotic treatment of C. rectus, so far, no beta-lactamase activity has been described and other than oxifloxacin, C. rectus appears to be sensitive to antibiotic treatment.22 29 30 The culture results in this case report did not show any antimicrobial resistances too, so that antibiotic therapy with the usual drugs could be prescribed. In overall, the prognosis of P. micra and C. rectus infections are good following an appropriate treatment.25
In conclusion, the high susceptibility to antibiotics and good prognosis would suggest that identification of the pathogen is not obligatory for accurate and resistance-oriented treatment. However, to prevent recurrence of infection, the surgical removal of infection focus is critical, as delay in treatment is associated with significantly increased morbidity and mortality.
Learning points
Parvimonas micra and Campylobacter rectus are both members of the oral microbiotic flora. Systemic infection is rare, however possible.
Since both bacterial strains are associated with chronic periodontitis, a dental focus should be considered in case of identification in systemic infections.
Parvimonas micra and Campylobacter rectus are highly susceptible to antibiotic treatment. To prevent recurrence of infection, identification and surgical removal of the source of infection is however critical.
Ethics statements
Patient consent for publication
Acknowledgments
We are grateful to H Notter, MD, M Valletti, MD and F Porchet who took care of the patient in the regional hospital, prior to referral to the University Hospital Zurich.
References
Footnotes
AA and SLvdB are joint first authors.
Contributors AA and SLvdB contributed to patient management and treatment and initial drafting the first version of the manuscript. AA, SLvdB, KS and DIK contributed to conception and design, writing the manuscript, critical revision of content and final approval of the manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Slankamenac K and Keller DI are joint senior authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.